

A New Three-Dimensional Classification of Proximal Tibiofibular Fractures: A Multicenter Study
- PMID: 34672099
- PMCID: PMC8654672
- DOI: 10.1111/os.13161
A New Three-Dimensional Classification of Proximal Tibiofibular Fractures: A Multicenter Study
Abstract
Objectives: To propose an updated definition of proximal tibia and fibula fracture (PTFF) and establish a three-dimensional (3D) structure-based classification of PTFF.
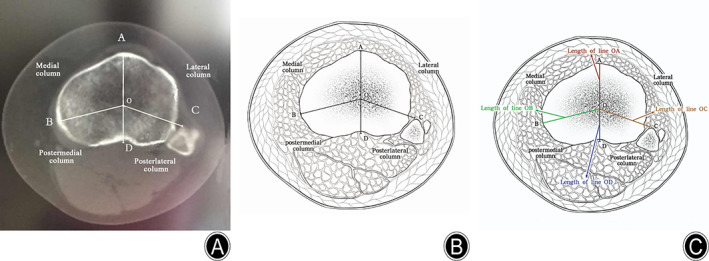
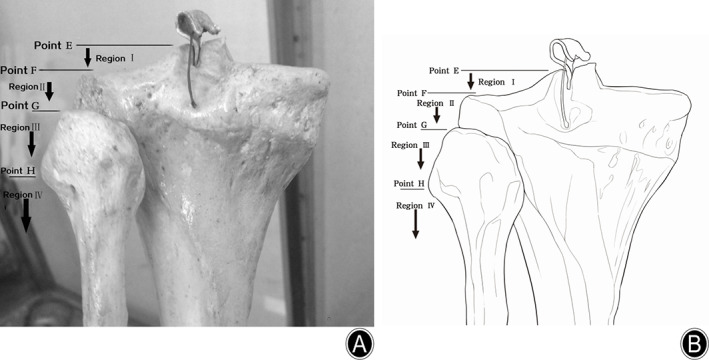
Methods: In total, 1358 adult patients (837 males and 521 females; 43.61 ± 15.13 years, 1364 affected knees) who were diagnosed with PTFF at the departments of orthopaedic surgery of four hospitals from January 2010 to December 2019 were enrolled. The new classification of PTFF, termed Wu classification, included three parts: classification of columns in the horizontal plane, regions in the frontal plane, and segments in the sagittal plane. All PTFFs were classified according to Schatzker, Luo, and Wu classification systems. Additionally, the incidence and characteristics of PTFFs were analyzed.
Results: The major internal structural fractures of PTFF were tibial plateau fracture (TPF) only (725, 53.15%), TPF and proximal fibular fracture (274, 20.09%), and isolated avulsion fracture of the posterior cruciate ligament (PCL) (189, 13.86%). Approximately a quarter of PTFF cases could not be classified using Schatzker or Luo classifications, but all PTFF cases could be classified using Wu classification. The most frequent PTFFs included all four columns in region IV, segment 2 (235, 17.23%); the posterolateral and posteromedial columns in region II, segment 2 (191, 14.00%); and the lateral and posterolateral columns in region IV, segment 2 (136, 9.97%). Isolated avulsion fracture of the anterior cruciate ligament (ACL) was categorized as three injury types, most of which involved the lateral and medial columns in region II, segment 1 (40/63, 64%). More than 97% of cases of isolated fractures of the PCL involved the posterolateral and posteromedial columns in region II, segment 2. The most frequent combined avulsion fracture of the ACL and PCL included all four columns in region II, segment 2 (18/24, 75%). All of the isolated avulsion fractures of the ACL were located in segment 1, and all those of the PCL in segment 2. The most common type of isolated proximal fibular fracture involved the posterolateral column in region III, segment 2 (23/26, 88%). The most frequent combined TPF and proximal fibular fracture involved all four columns in region IV, segment 2 (107/274, 39.05%).
Conclusions: All cases of PTFF could be classified by the new 3D Wu classification which should be beneficial for clinical diagnosis, guidance of treatment, statistical analysis, academic communication, and prognosis, and the most frequent PTFF involved all four columns in region IV, segment 2.
Keywords: Classification; Fibula; Fracture; Knee joint; Tibia.
© 2021 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures






References
-
- Bernholt DL, DePhillipo NN, Crawford MD, Aman ZS, Grantham WJ, LaPrade RF. Incidence of displaced posterolateral tibial plateau and lateral femoral condyle impaction fractures in the setting of primary anterior cruciate ligament tear. Am J Sports Med, 2020, 48: 545–553. - PubMed
-
- Yi Z, Hui S, Binbin Z, et al. A new strategy to fix posterolateral depression in tibial plateau fractures: introduction of a new modified Frosch approach and a "barrel hoop plate" technique. Injury, 2020, 51: 723–734. - PubMed
-
- Xie X, Zhan Y, Wang Y, Lucas JF, Zhang Y, Luo C. Comparative analysis of mechanism‐associated 3‐dimensional tibial plateau fracture patterns. J Bone Joint Surg Am, 2020, 102: 410–418. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
