

Declining HIV incidence in sub-Saharan Africa: a systematic review and meta-analysis of empiric data
- PMID: 34672104
- PMCID: PMC8528667
- DOI: 10.1002/jia2.25818
Declining HIV incidence in sub-Saharan Africa: a systematic review and meta-analysis of empiric data
Abstract
Introduction: UNAIDS models suggest HIV incidence is declining in sub-Saharan Africa. The objective of this study was to assess whether modelled trends are supported by empirical evidence.
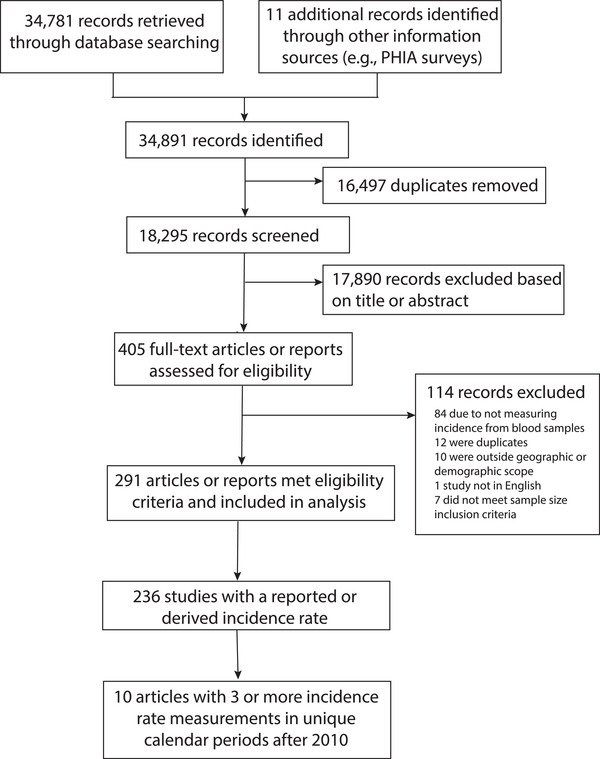
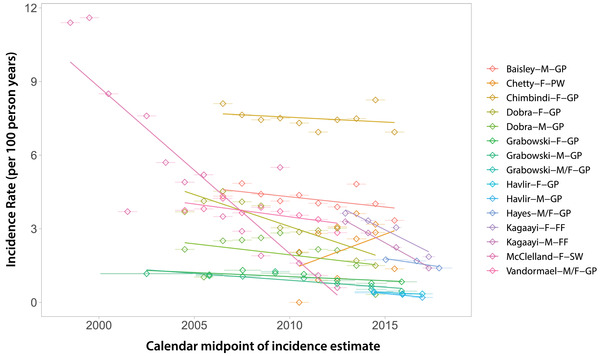
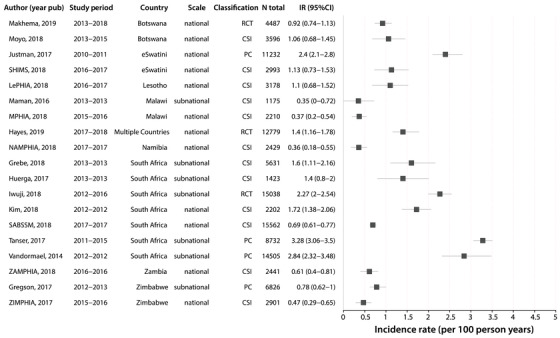
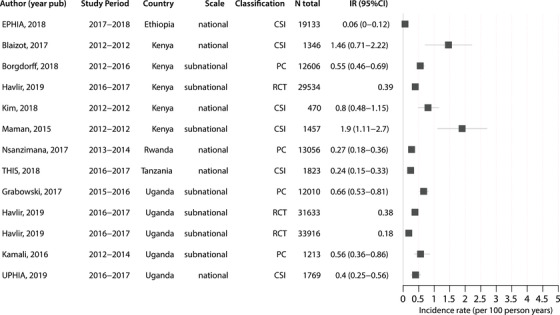
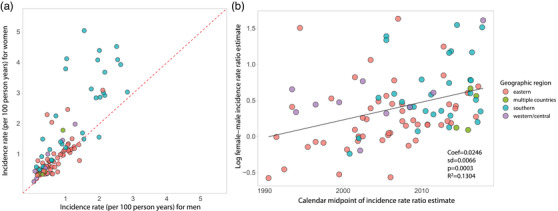
Methods: We conducted a systematic review and meta-analysis of adult HIV incidence data from sub-Saharan Africa by searching Embase, Scopus, PubMed and OVID databases and technical reports published between 1 January 2010 and 23 July 2019. We included prospective and cross-sectional studies that directly measured incidence from blood samples. Incidence data were abstracted according to population risk group, geographic location, sex, intervention arm and calendar period. Weighted regression models were used to assess incidence trends across general population studies by sex. We also identified studies reporting greater than or equal to three incidence measurements since 2010 and assessed trends within them.
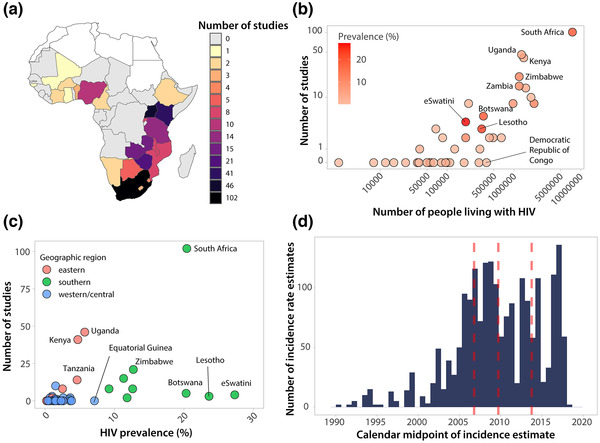
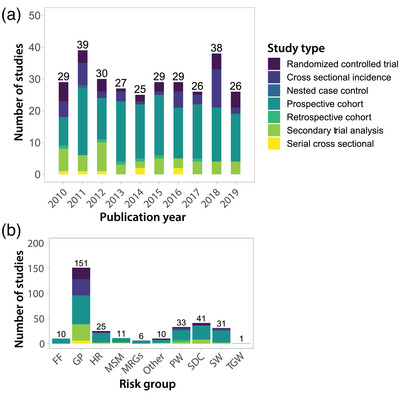
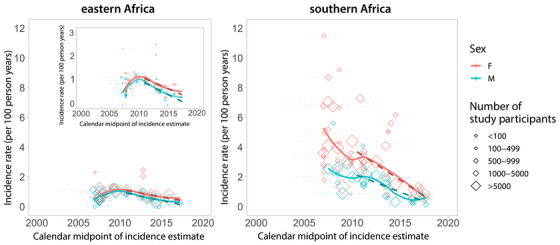
Results: Total 291 studies, including 22 sub-Saharan African countries, met inclusion criteria. Most studies were conducted in South Africa (n = 102), Uganda (n = 46) and Kenya (n = 41); there were 26 countries with no published incidence data, most in western and central Africa. Data were most commonly derived from prospective observational studies (n = 163; 56%) and from geographically defined populations with limited demographic or risk-based enrolment criteria other than age (i.e., general population studies; n = 151; 52%). Across general population studies, average annual incidence declines since 2010 were 0.12/100 person-years (95% CI: 0.06-0.18; p = 0.001) among men and 0.10/100 person-years (95% CI: -0.02-0.22; p = 0.093) among women in eastern Africa, and 0.25/100 person-years (95% CI: 0.17-034; p < 0.0001) among men and 0.42/100 person-years (95% CI: 0.23-0.62; p = 0.0002) among women in southern Africa. In nine of 10 studies with multiple measurements, incidence declined over time, including in two studies of key populations. Across all population risk groups, the highest HIV incidence estimates were observed among men who have sex with men, with rates ranging from 1.0 to 15.4/100 person-years. Within general population studies, incidence was typically higher in women than men with a median female-to-male incidence rate ratio of 1.47 (IQR: 1.11 to 1.83) with evidence of a growing sex disparity over time.
Conclusions: Empirical incidence data show the rate of new HIV infections is declining in eastern and southern Africa. However, recent incidence data are non-existent or very limited for many countries and key populations.
Keywords: Africa; HIV epidemiology; HIV incidence; HIV prevention; clinical trials; cohort studies; key and vulnerable populations.
© 2021 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- 2020 Global AIDS Update ‐ Seizing the Moment ‐ Tackling Entrenched Inequalities to End Epidemics [Internet]. UNAIDS. [cited 2020 Oct 7]. Available from: https://www.unaids.org/en/resources/documents/2020/global‐aids‐report
-
- Kates J, Wexler A. Donor Government Funding for HIV in Low‐ and Middle‐Income Countries in 2019. UNAIDS; 2020.
-
- Galvani AP, Pandey A, Fitzpatrick MC, Medlock J, Gray GE. Defining control of HIV epidemics. Lancet HIV. 2018;. 5:e667–70. - PubMed
-
- GBD 2017 HIV collaborators . Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV. 2019;. 6:e831–59. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
