

Enhanced medical diagnosis for dOCTors: a perspective of optical coherence tomography
- PMID: 34672145
- PMCID: PMC8528212
- DOI: 10.1117/1.JBO.26.10.100601
Enhanced medical diagnosis for dOCTors: a perspective of optical coherence tomography
Abstract
Significance: After three decades, more than 75,000 publications, tens of companies being involved in its commercialization, and a global market perspective of about USD 1.5 billion in 2023, optical coherence tomography (OCT) has become one of the fastest successfully translated imaging techniques with substantial clinical and economic impacts and acceptance.
Aim: Our perspective focuses on disruptive forward-looking innovations and key technologies to further boost OCT performance and therefore enable significantly enhanced medical diagnosis.
Approach: A comprehensive review of state-of-the-art accomplishments in OCT has been performed.
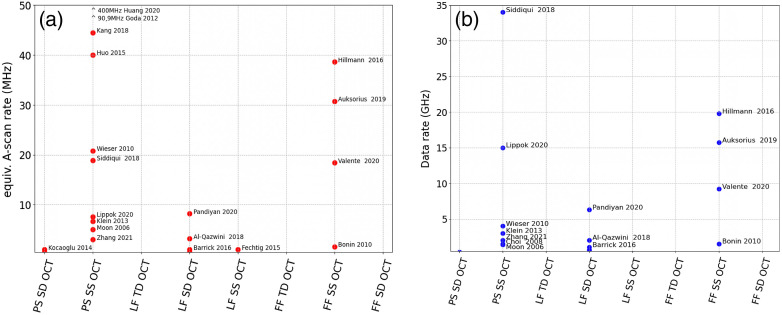
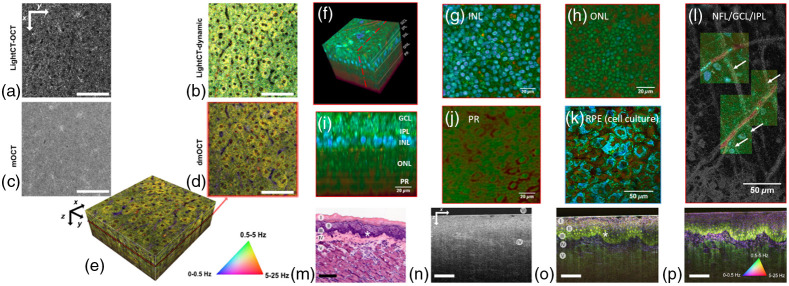
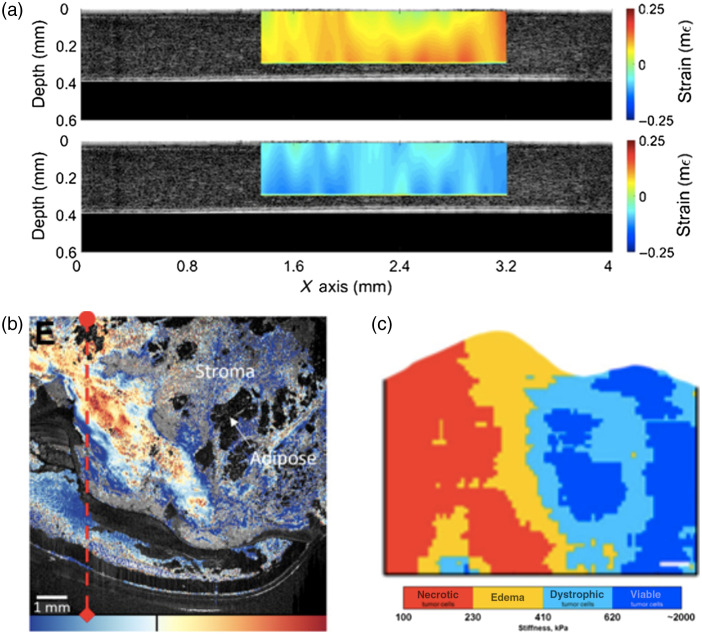
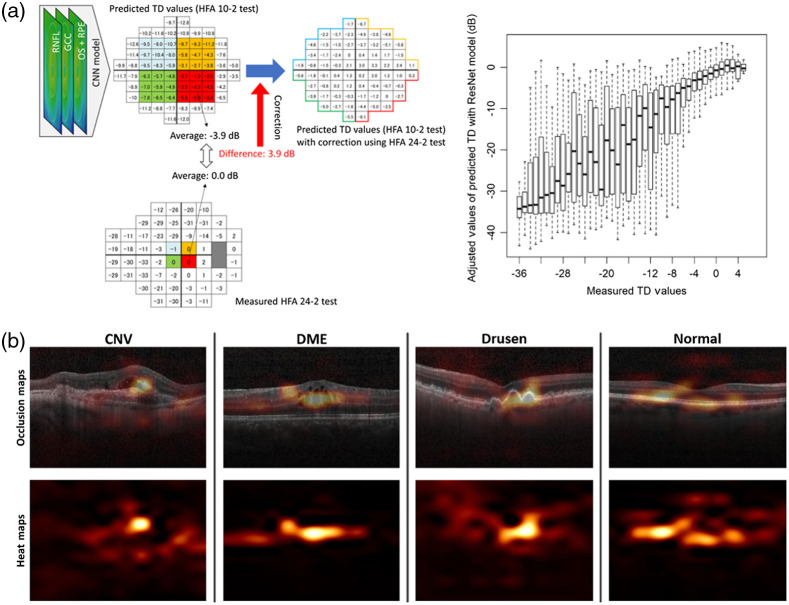
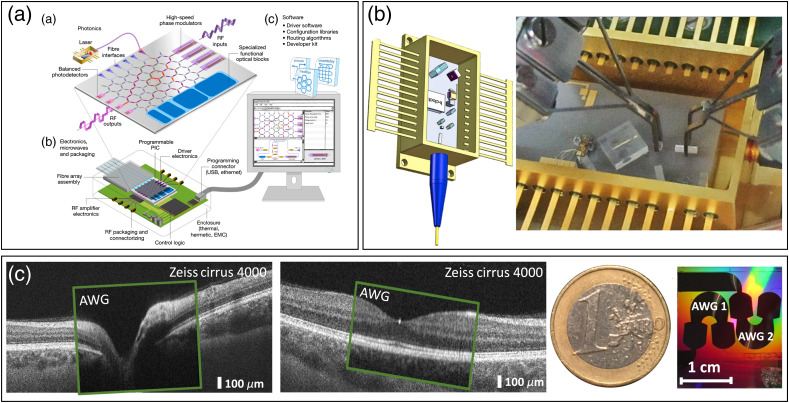
Results: The most disruptive future OCT innovations include imaging resolution and speed (single-beam raster scanning versus parallelization) improvement, new implementations for dual modality or even multimodality systems, and using endogenous or exogenous contrast in these hybrid OCT systems targeting molecular and metabolic imaging. Aside from OCT angiography, no other functional or contrast enhancing OCT extension has accomplished comparable clinical and commercial impacts. Some more recently developed extensions, e.g., optical coherence elastography, dynamic contrast OCT, optoretinography, and artificial intelligence enhanced OCT are also considered with high potential for the future. In addition, OCT miniaturization for portable, compact, handheld, and/or cost-effective capsule-based OCT applications, home-OCT, and self-OCT systems based on micro-optic assemblies or photonic integrated circuits will revolutionize new applications and availability in the near future. Finally, clinical translation of OCT including medical device regulatory challenges will continue to be absolutely essential.
Conclusions: With its exquisite non-invasive, micrometer resolution depth sectioning capability, OCT has especially revolutionized ophthalmic diagnosis and hence is the fastest adopted imaging technology in the history of ophthalmology. Nonetheless, OCT has not been completely exploited and has substantial growth potential-in academics as well as in industry. This applies not only to the ophthalmic application field, but also especially to the original motivation of OCT to enable optical biopsy, i.e., the in situ imaging of tissue microstructure with a resolution approaching that of histology but without the need for tissue excision.
Keywords: contrast enhanced OCT; functional OCT; miniaturized OCT; multimodal OCT; multimodal OCT endoscopy; non-linear optical microscopy; optical coherence tomography; photoacoustic imaging.
Figures
Similar articles
-
Methods and applications of full-field optical coherence tomography: a review.J Biomed Opt. 2022 May;27(5):050901. doi: 10.1117/1.JBO.27.5.050901. J Biomed Opt. 2022. PMID: 35596250 Free PMC article. Review.
-
Optical coherence tomography today: speed, contrast, and multimodality.J Biomed Opt. 2014;19(7):071412. doi: 10.1117/1.JBO.19.7.071412. J Biomed Opt. 2014. PMID: 25079820 Review.
-
Fiber-based photoacoustic remote sensing microscopy and spectral-domain optical coherence tomography with a dual-function 1050-nm interrogation source.J Biomed Opt. 2021 Jun;26(6):066502. doi: 10.1117/1.JBO.26.6.066502. J Biomed Opt. 2021. PMID: 34164968 Free PMC article.
-
Optical Coherence Tomography for Ophthalmology Imaging.Adv Exp Med Biol. 2021;3233:197-216. doi: 10.1007/978-981-15-7627-0_10. Adv Exp Med Biol. 2021. PMID: 34053029
-
Optical Coherence Tomography (OCT): A Brief Look at the Uses and Technological Evolution of Ophthalmology.Medicina (Kaunas). 2023 Dec 3;59(12):2114. doi: 10.3390/medicina59122114. Medicina (Kaunas). 2023. PMID: 38138217 Free PMC article. Review.
Cited by
-
Contrast-enhanced Micro-CT 3D visualization of cell distribution in hydrated human cornea.Heliyon. 2024 Feb 3;10(3):e25828. doi: 10.1016/j.heliyon.2024.e25828. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38356495 Free PMC article.
-
Compression OCT-elastography combined with speckle-contrast analysis as an approach to the morphological assessment of breast cancer tissue.Biomed Opt Express. 2023 May 31;14(6):3037-3056. doi: 10.1364/BOE.489021. eCollection 2023 Jun 1. Biomed Opt Express. 2023. PMID: 37342703 Free PMC article.
-
Cone Density Is Correlated to Outer Segment Length and Retinal Thickness in the Human Foveola.Invest Ophthalmol Vis Sci. 2023 Dec 1;64(15):11. doi: 10.1167/iovs.64.15.11. Invest Ophthalmol Vis Sci. 2023. PMID: 38064229 Free PMC article.
-
Cross-attention learning enables real-time nonuniform rotational distortion correction in OCT.Biomed Opt Express. 2023 Dec 19;15(1):319-335. doi: 10.1364/BOE.512337. eCollection 2024 Jan 1. Biomed Opt Express. 2023. PMID: 38223193 Free PMC article.
-
Quantitative evaluation of the site-dependent cell viability in three-dimensional hepatocyte spheroids based on dynamic optical coherence tomography.J Biomed Opt. 2025 Mar;30(3):035003. doi: 10.1117/1.JBO.30.3.035003. Epub 2025 Mar 14. J Biomed Opt. 2025. PMID: 40134833 Free PMC article.
References
-
- Drexler W., Fujimoto J. G., Optical Coherence Tomography: Technology and Applications, 2nd ed., Springer Publishing, Switzerland: (2015).
-
- Fercher A. F., Roth E., Eds., Ophthalmic Laser Interferometer (1986).
