

Cost-effectiveness Evaluation of the 2021 US Preventive Services Task Force Recommendation for Lung Cancer Screening
- PMID: 34673885
- PMCID: PMC8532037
- DOI: 10.1001/jamaoncol.2021.4942
Cost-effectiveness Evaluation of the 2021 US Preventive Services Task Force Recommendation for Lung Cancer Screening
Abstract
Importance: The US Preventive Services Task Force (USPSTF) issued its 2021 recommendation on lung cancer screening, which lowered the starting age for screening from 55 to 50 years and the minimum cumulative smoking exposure from 30 to 20 pack-years relative to its 2013 recommendation. Although costs are expected to increase because of the expanded screening eligibility criteria, it is unknown whether the new guidelines for lung cancer screening are cost-effective.
Objective: To evaluate the cost-effectiveness of the 2021 USPSTF recommendation for lung cancer screening compared with the 2013 recommendation and to explore the cost-effectiveness of 6 alternative screening strategies that maintained a minimum cumulative smoking exposure of 20 pack-years and an ending age for screening of 80 years but varied the starting ages for screening (50 or 55 years) and the number of years since smoking cessation (≤15, ≤20, or ≤25).
Design, setting, and participants: A comparative cost-effectiveness analysis using 4 independently developed microsimulation models that shared common inputs to assess the population-level health benefits and costs of the 2021 recommended screening strategy and 6 alternative screening strategies compared with the 2013 recommended screening strategy. The models simulated a 1960 US birth cohort. Simulated individuals entered the study at age 45 years and were followed up until death or age 90 years, corresponding to a study period from January 1, 2005, to December 31, 2050.
Exposures: Low-dose computed tomography in lung cancer screening programs with a minimum cumulative smoking exposure of 20 pack-years.
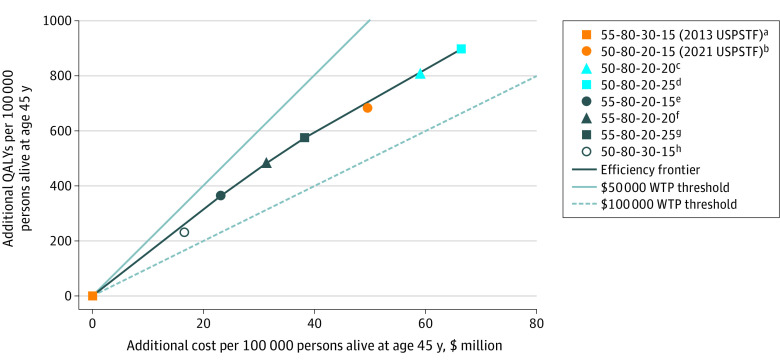
Main outcomes and measures: Incremental cost-effectiveness ratio (ICER) per quality-adjusted life-year (QALY) of the 2021 vs 2013 USPSTF lung cancer screening recommendations as well as 6 alternative screening strategies vs the 2013 USPSTF screening strategy. Strategies with a mean ICER lower than $100 000 per QALY were deemed cost-effective.
Results: The 2021 USPSTF recommendation was estimated to be cost-effective compared with the 2013 recommendation, with a mean ICER of $72 564 (range across 4 models, $59 493-$85 837) per QALY gained. The 2021 recommendation was not cost-effective compared with 6 alternative strategies that used the 20 pack-year criterion. Strategies associated with the most cost-effectiveness included those that expanded screening eligibility to include a greater number of former smokers who had not smoked for a longer duration (ie, ≤20 years and ≤25 years since smoking cessation vs ≤15 years since smoking cessation). In particular, the strategy that screened former smokers who quit within the past 25 years and began screening at age 55 years was associated with screening coverage closest to that of the 2021 USPSTF recommendation yet yielded greater cost-effectiveness, with a mean ICER of $66 533 (range across 4 models, $55 693-$80 539).
Conclusions and relevance: This economic evaluation found that the 2021 USPSTF recommendation for lung cancer screening was cost-effective; however, alternative screening strategies that maintained a minimum cumulative smoking exposure of 20 pack-years but included individuals who quit smoking within the past 25 years may be more cost-effective and warrant further evaluation.
Conflict of interest statement
Figures
Comment in
-
The Long, Slow Road to Lung Cancer Cure.JAMA Oncol. 2021 Dec 1;7(12):1765-1767. doi: 10.1001/jamaoncol.2021.4711. JAMA Oncol. 2021. PMID: 34673896 No abstract available.
References
-
- U.S. Preventive Services Task Force . Final recommendation statement. lung cancer: screening. U.S. Preventive Services Task Force. March 9, 2021. Accessed March 9, 2021. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung...
-
- Meza R, Jeon J, Toumazis I, et al. Evaluation of the Benefits and Harms of Lung Cancer Screening With Low-Dose Computed Tomography: A Collaborative Modeling Study for the U.S. Preventive Services Task Force. Agency for Healthcare Research and Quality; 2021. Evidence syntheses 198tr. Report 20-05266-EF-2. March 2021. Accessed March 9, 2021. https://www.ncbi.nlm.nih.gov/books/NBK568586/ - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
