

Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non-Small Cell Lung Cancer in the US
- PMID: 34673888
- PMCID: PMC8532041
- DOI: 10.1001/jamaoncol.2021.4932
Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non-Small Cell Lung Cancer in the US
Abstract
Importance: Updated estimates of non-small cell lung cancer (NSCLC) in the US are needed.
Objective: To calculate the most recent epidemiologic estimates of NSCLC in the US.
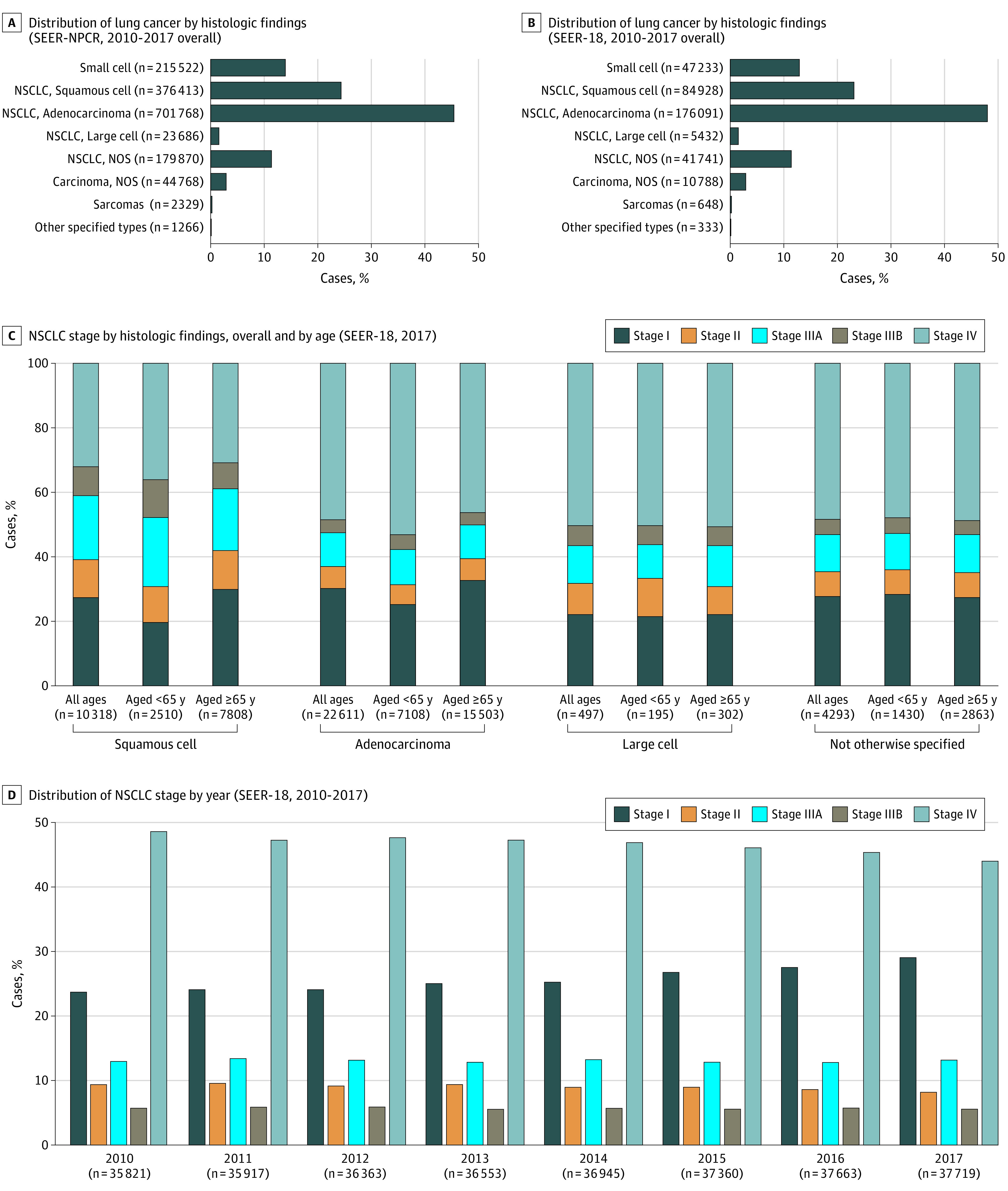
Design, setting, and participants: This cross-sectional epidemiological analysis used the most recently released data from US cancer registries. The population-based US Cancer Statistics (USCS) database (2010-2017), comprised of the Surveillance, Epidemiology, and End Results (SEER) program and the National Program of Cancer Registries (NPCR) (collectively, SEER-NPCR) provided the NSCLC incidence estimate. The SEER-18 database provided data for incidence, prevalence, survival, and initial treatment by NSCLC stage. Adults aged 18 years or older diagnosed with NSCLC identified by International Classification of Diseases for Oncology, Third Edition, morphology codes were included.
Main outcomes and measures: Annual age-adjusted NSCLC incidence per 100 000 persons; annual prevalence per 100 000 persons; survival rate; initial treatment. Due to database release delays, incidence data were available through 2017, and other parameters through 2016. The analysis was conducted from June 2020 to July 2020.
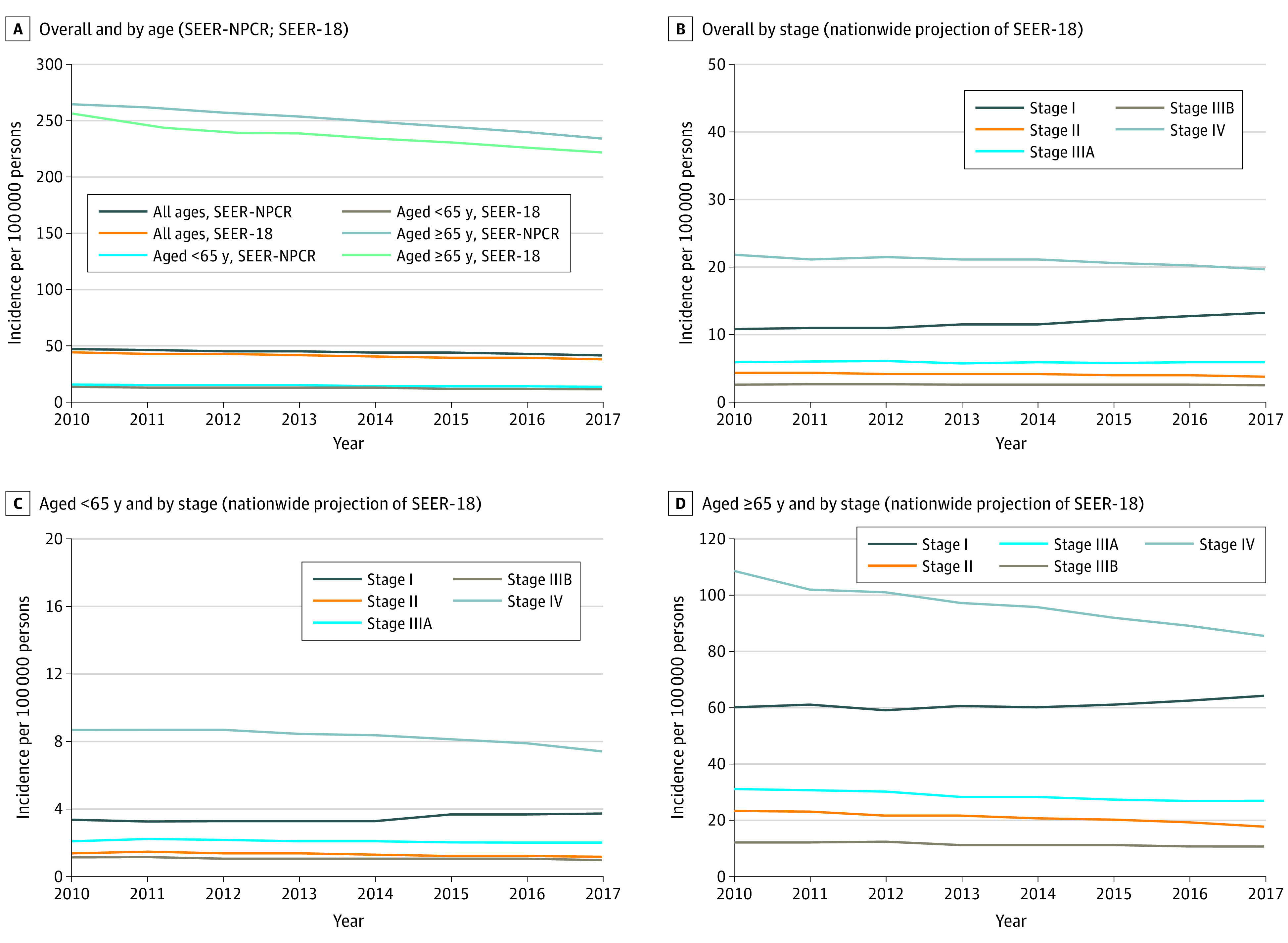
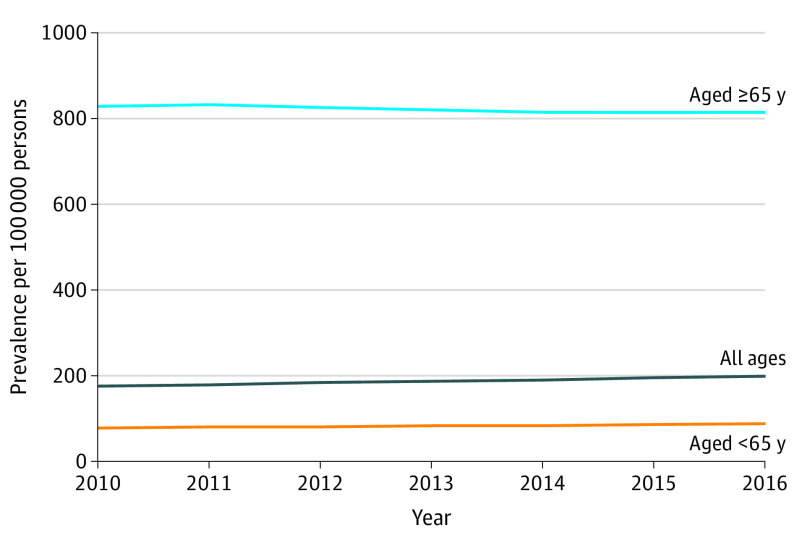
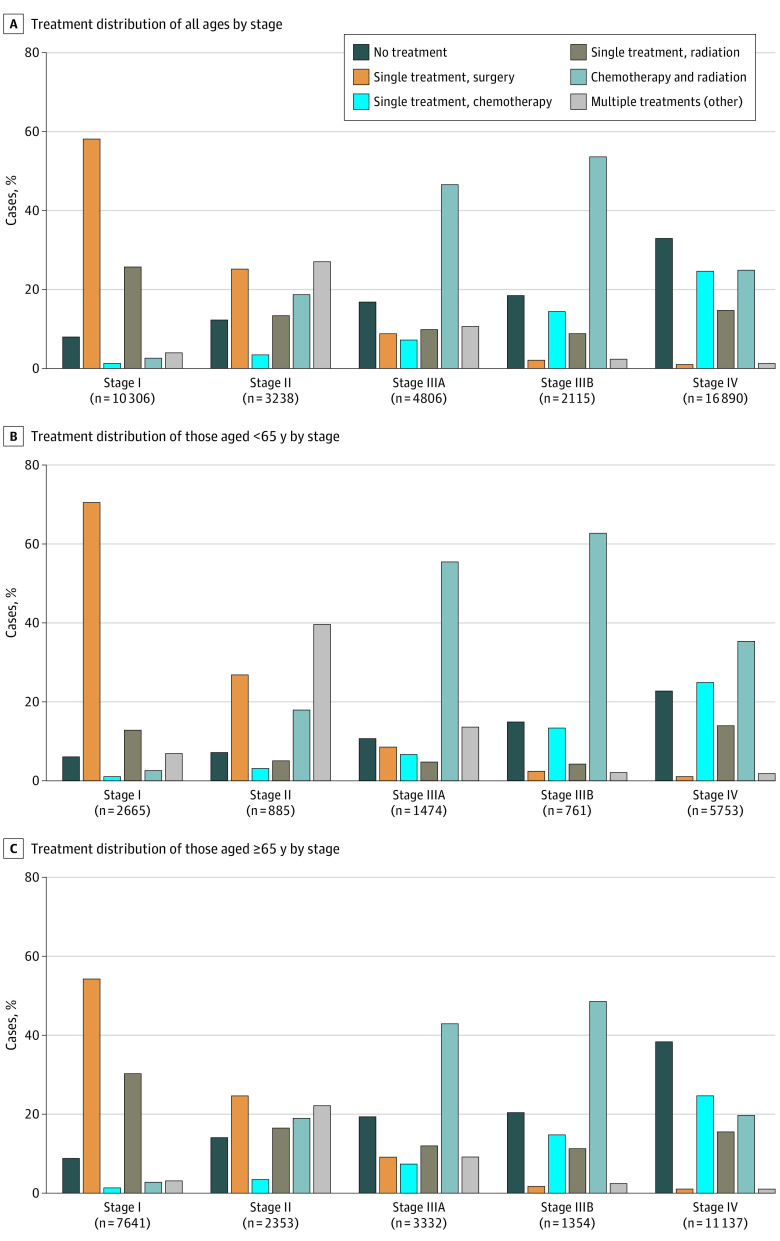
Results: There were 1.28 million new NSCLC cases recorded during 2010 to 2017 in the US (SEER-NPCR: 53% male; 67% ≥ 65 years). From 2010 to 2017, NSCLC incidence per 100 000 decreased from 46.4 to 40.9 overall (age <65 years: 15.5 to 13.5; age ≥65 years: 259.9 to 230.0); the incidence of stage II, IIIA, and IIIB NSCLC was stable, and stage IV decreased slightly from 21.7 to 19.6, whereas stage I incidence increased from 10.8 to 13.2. From 2010 to 2016, NSCLC prevalence per 100 000 increased from 175.3 to 198.3 (nationwide projection of SEER-18); prevalence increased among younger patients (77.5 to 87.9) but decreased among older patients (825.1 to 812.4). Period survival analysis found that 26.4% of patients survived 5 years, which is higher than previously reported. The proportion of stage I NSCLC treated with radiation as single initial treatment rose markedly from 14.7% in 2010 to 25.7% in 2016. Patients with stage IV NSCLC aged 65 years or older were most likely to be untreated (38.3%).
Conclusions and relevance: The findings of this cross-sectional epidemiological analysis suggest that the increased incidence of stage I NSCLC at diagnosis likely reflected improved evaluation of incidental nodules. A smaller proportion of patients aged 65 years or older with stage IV NSCLC were treated. Earlier detection and availability of effective treatments may underlie increased overall NSCLC prevalence, and higher than previously reported survival.
Conflict of interest statement
Figures
Comment in
-
The Long, Slow Road to Lung Cancer Cure.JAMA Oncol. 2021 Dec 1;7(12):1765-1767. doi: 10.1001/jamaoncol.2021.4711. JAMA Oncol. 2021. PMID: 34673896 No abstract available.
References
-
- American Cancer Society . Facts & Figures 2019. Accessed June 13, 2020. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-...
-
- Diwanji TP, Mohindra P, Vyfhuis M, et al. . Advances in radiotherapy techniques and delivery for non-small cell lung cancer: benefits of intensity-modulated radiation therapy, proton therapy, and stereotactic body radiation therapy. Transl Lung Cancer Res. 2017;6(2):131-147. doi:10.21037/tlcr.2017.04.04 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
