

Effect of 12 mg vs 6 mg of Dexamethasone on the Number of Days Alive Without Life Support in Adults With COVID-19 and Severe Hypoxemia: The COVID STEROID 2 Randomized Trial
- PMID: 34673895
- PMCID: PMC8532039
- DOI: 10.1001/jama.2021.18295
Effect of 12 mg vs 6 mg of Dexamethasone on the Number of Days Alive Without Life Support in Adults With COVID-19 and Severe Hypoxemia: The COVID STEROID 2 Randomized Trial
Erratum in
-
Incorrect Wording in 2 Places.JAMA. 2021 Dec 14;326(22):2333. doi: 10.1001/jama.2021.21529. JAMA. 2021. PMID: 34905047 Free PMC article. No abstract available.
-
Incorrect Equivalent Dose and P Values in Figure 3.JAMA. 2022 Jan 18;327(3):286. doi: 10.1001/jama.2021.24153. JAMA. 2022. PMID: 35040905 Free PMC article. No abstract available.
Abstract
Importance: A daily dose with 6 mg of dexamethasone is recommended for up to 10 days in patients with severe and critical COVID-19, but a higher dose may benefit those with more severe disease.
Objective: To assess the effects of 12 mg/d vs 6 mg/d of dexamethasone in patients with COVID-19 and severe hypoxemia.
Design, setting, and participants: A multicenter, randomized clinical trial was conducted between August 2020 and May 2021 at 26 hospitals in Europe and India and included 1000 adults with confirmed COVID-19 requiring at least 10 L/min of oxygen or mechanical ventilation. End of 90-day follow-up was on August 19, 2021.
Interventions: Patients were randomized 1:1 to 12 mg/d of intravenous dexamethasone (n = 503) or 6 mg/d of intravenous dexamethasone (n = 497) for up to 10 days.
Main outcomes and measures: The primary outcome was the number of days alive without life support (invasive mechanical ventilation, circulatory support, or kidney replacement therapy) at 28 days and was adjusted for stratification variables. Of the 8 prespecified secondary outcomes, 5 are included in this analysis (the number of days alive without life support at 90 days, the number of days alive out of the hospital at 90 days, mortality at 28 days and at 90 days, and ≥1 serious adverse reactions at 28 days).
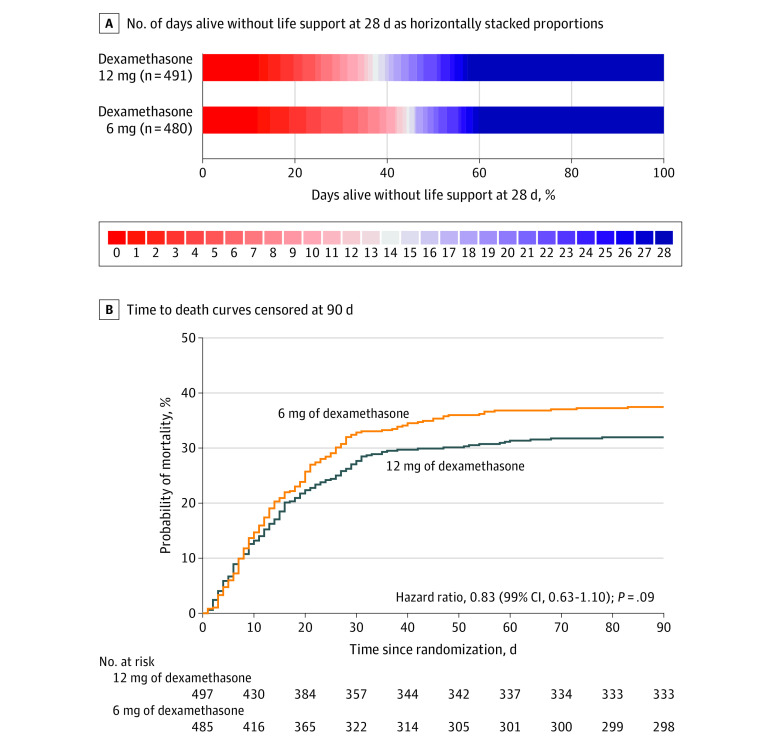
Results: Of the 1000 randomized patients, 982 were included (median age, 65 [IQR, 55-73] years; 305 [31%] women) and primary outcome data were available for 971 (491 in the 12 mg of dexamethasone group and 480 in the 6 mg of dexamethasone group). The median number of days alive without life support was 22.0 days (IQR, 6.0-28.0 days) in the 12 mg of dexamethasone group and 20.5 days (IQR, 4.0-28.0 days) in the 6 mg of dexamethasone group (adjusted mean difference, 1.3 days [95% CI, 0-2.6 days]; P = .07). Mortality at 28 days was 27.1% in the 12 mg of dexamethasone group vs 32.3% in the 6 mg of dexamethasone group (adjusted relative risk, 0.86 [99% CI, 0.68-1.08]). Mortality at 90 days was 32.0% in the 12 mg of dexamethasone group vs 37.7% in the 6 mg of dexamethasone group (adjusted relative risk, 0.87 [99% CI, 0.70-1.07]). Serious adverse reactions, including septic shock and invasive fungal infections, occurred in 11.3% in the 12 mg of dexamethasone group vs 13.4% in the 6 mg of dexamethasone group (adjusted relative risk, 0.83 [99% CI, 0.54-1.29]).
Conclusions and relevance: Among patients with COVID-19 and severe hypoxemia, 12 mg/d of dexamethasone compared with 6 mg/d of dexamethasone did not result in statistically significantly more days alive without life support at 28 days. However, the trial may have been underpowered to identify a significant difference.
Trial registration: ClinicalTrials.gov Identifier: NCT04509973 and ctri.nic.in Identifier: CTRI/2020/10/028731.
Conflict of interest statement
Figures


Comment in
-
Glucocorticoid Dose in COVID-19: Lessons for Clinical Trials During a Pandemic.JAMA. 2021 Nov 9;326(18):1801-1802. doi: 10.1001/jama.2021.16438. JAMA. 2021. PMID: 34673891 No abstract available.
-
Dexamethasone and Number of Days Alive Without Life Support in Adults With COVID-19 and Severe Hypoxemia.JAMA. 2022 Feb 15;327(7):682-683. doi: 10.1001/jama.2021.24532. JAMA. 2022. PMID: 35166808 No abstract available.
-
Dexamethasone and Number of Days Alive Without Life Support in Adults With COVID-19 and Severe Hypoxemia.JAMA. 2022 Feb 15;327(7):682. doi: 10.1001/jama.2021.24525. JAMA. 2022. PMID: 35166809 No abstract available.
-
Dexamethasone and Number of Days Alive Without Life Support in Adults With COVID-19 and Severe Hypoxemia.JAMA. 2022 Feb 15;327(7):682. doi: 10.1001/jama.2021.24522. JAMA. 2022. PMID: 35166810 No abstract available.
-
In COVID-19 with hypoxemia, 12 vs. 6 mg/d of dexamethasone did not increase days alive without life support.Ann Intern Med. 2022 Mar;175(3):JC33. doi: 10.7326/J22-0001. Epub 2022 Mar 1. Ann Intern Med. 2022. PMID: 35226531
References
-
- Sterne JAC, Murthy S, Diaz JV, et al. ; WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group . Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 2020;324(13):1330-1341. doi: 10.1001/jama.2020.17023 - DOI - PMC - PubMed
-
- Angus DC, Derde L, Al-Beidh F, et al. ; Writing Committee for the REMAP-CAP Investigators . Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: the REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial. JAMA. 2020;324(13):1317-1329. doi: 10.1001/jama.2020.17022 - DOI - PMC - PubMed
