

Association of Deficits Identified by Geriatric Assessment With Deterioration of Health-Related Quality of Life in Patients Treated for Head and Neck Cancer
- PMID: 34673914
- PMCID: PMC8532038
- DOI: 10.1001/jamaoto.2021.2837
Association of Deficits Identified by Geriatric Assessment With Deterioration of Health-Related Quality of Life in Patients Treated for Head and Neck Cancer
Abstract
Importance: Accumulation of geriatric deficits, leading to an increased frailty state, makes patients susceptible for decline in health-related quality of life (HRQOL) after treatment for head and neck cancer (HNC).
Objective: To assess the association of single and accumulated geriatric deficits with HRQOL decline in patients after treatment for HNC.
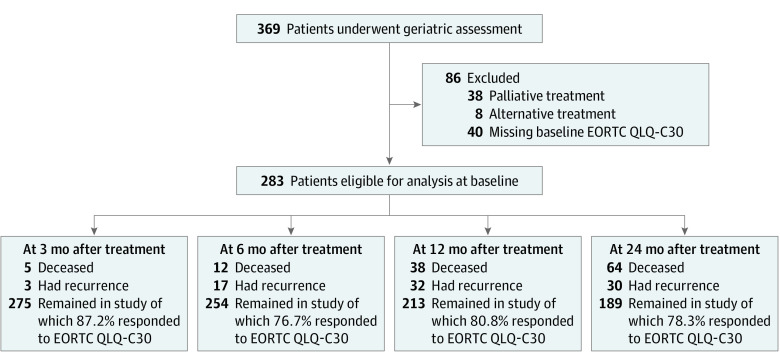
Design, setting, and participants: Between October 2014 and May 2016, patients at a tertiary referral center were included in the Oncological Life Study (OncoLifeS), a prospective data biobank, and followed up for 2 years. A consecutive series of 369 patients with HNC underwent geriatric assessment at baseline; a cohort of 283 patients remained eligible for analysis, and after 2 years, 189 patients remained in the study. Analysis was performed between March and November 2020.
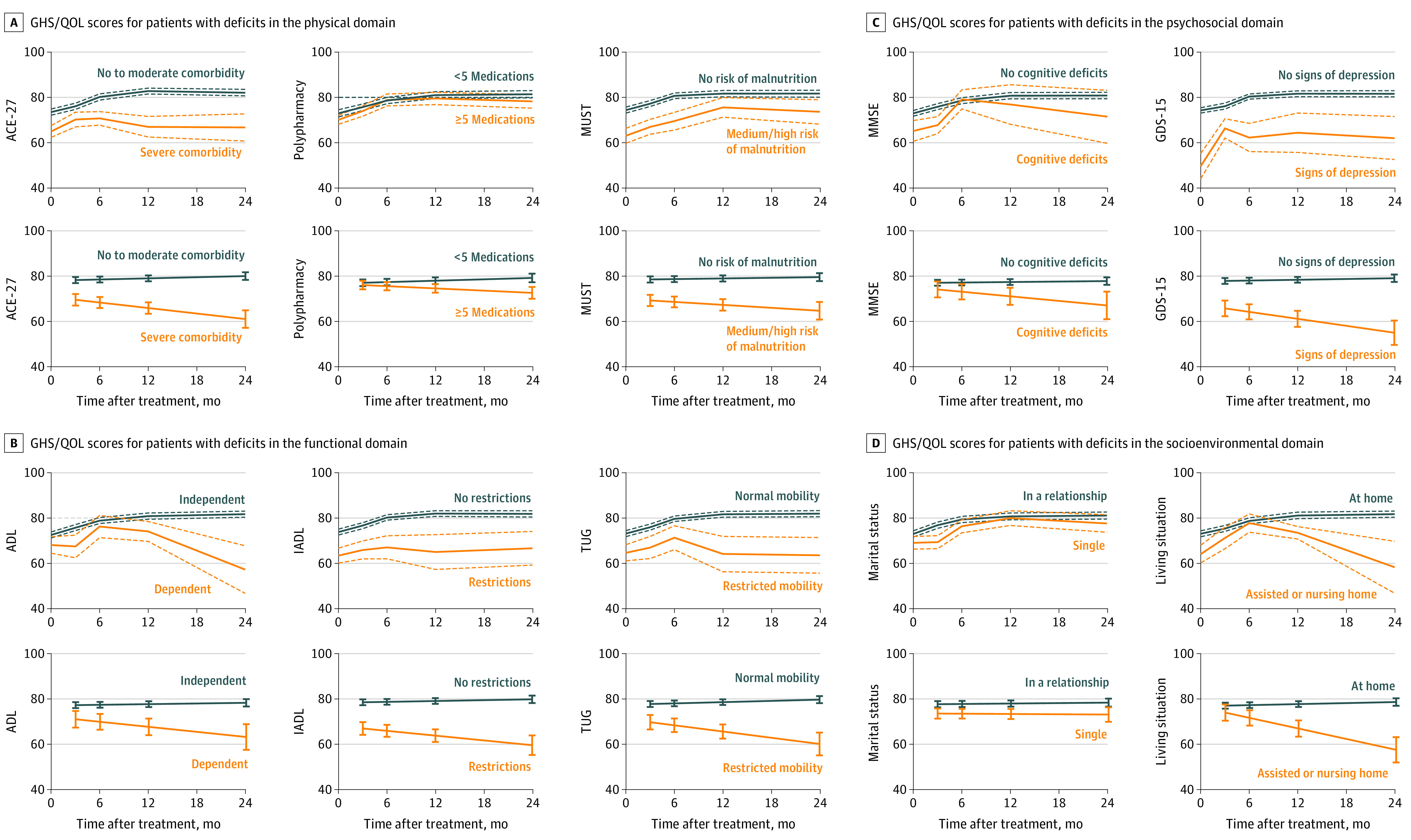
Interventions or exposures: Geriatric assessment included scoring of the Adult Comorbidity Evaluation 27, polypharmacy, Malnutrition Universal Screening Tool, Activities of Daily Living, Instrumental Activities of Daily Living (IADL), Timed Up & Go, Mini-Mental State Examination, 15-item Geriatric Depression Scale, marital status, and living situation.
Main outcomes and measures: The primary outcome measure was the Global Health Status/Quality of Life (GHS/QOL) scale of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Differences between patients were evaluated using linear mixed models at 3 months after treatment (main effects, β [95% CI]) and declining course per year during follow-up (interaction × time, β [95% CI]), adjusted for baseline GHS/QOL scores, and age, sex, stage, and treatment modality.
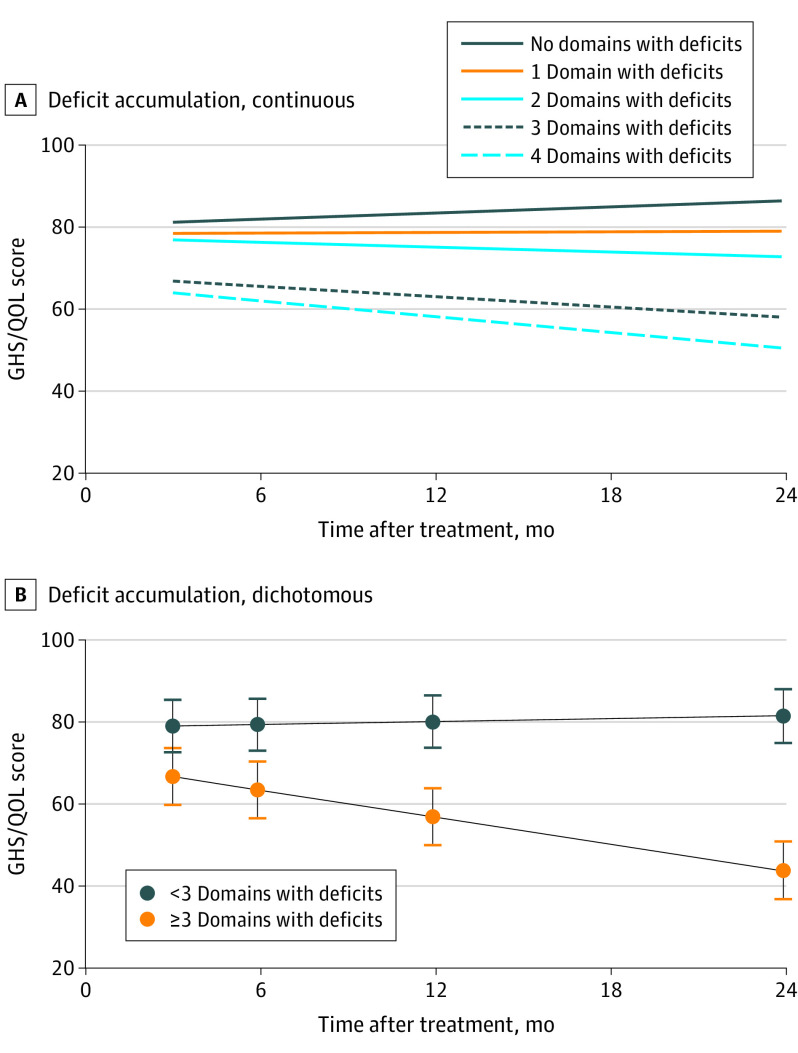
Results: Among the 283 patients eligible for analysis, the mean (SD) age was 68.3 (10.9) years, and 193 (68.2%) were male. Severe comorbidity (β = -7.00 [-12.43 to 1.56]), risk of malnutrition (β = -6.18 [-11.55 to -0.81]), and IADL restrictions (β = -10.48 [-16.39 to -4.57]) were associated with increased GHS/QOL decline at 3 months after treatment. Severe comorbidity (β = -4.90 [-9.70 to -0.10]), IADL restrictions (β = -5.36 [-10.50 to -0.22]), restricted mobility (β = -6.78 [-12.81 to -0.75]), signs of depression (β = -7.08 [-13.10 to -1.06]), and living with assistance or in a nursing home (β = -8.74 [-15.75 to -1.73]) were associated with further GHS/QOL decline during follow-up. Accumulation of domains with geriatric deficits was a major significant factor for GHS/QOL decline at 3 months after treatment (per deficient domain β = -3.17 [-5.04 to -1.30]) and deterioration during follow-up (per domain per year β = -2.74 [-4.28 to -1.20]).
Conclusions and relevance: In this prospective cohort study, geriatric deficits were significantly associated with HRQOL decline after treatment for HNC. Therefore, geriatric assessment may aid decision-making, indicate interventions, and reduce loss of HRQOL.
Trial registration: trialregister.nl Identifier: NL7839.
Conflict of interest statement
Figures
References
-
- van Deudekom FJ, Schimberg AS, Kallenberg MH, Slingerland M, van der Velden LA, Mooijaart SP. Functional and cognitive impairment, social environment, frailty and adverse health outcomes in older patients with head and neck cancer, a systematic review. Oral Oncol. 2017;64:27-36. doi:10.1016/j.oraloncology.2016.11.013 - DOI - PubMed
-
- Bray F, Soerjomataram I. The changing global burden of cancer: transitions in human development and implications for cancer prevention and control. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, eds. Cancer: Disease Control Priorities. 3rd ed. International Bank for Reconstruction and Development/The World Bank; 2015:23-44. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
