

Racial and Ethnic Disparities in Rates of COVID-19-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death in the United States From March 2020 to February 2021
- PMID: 34673962
- PMCID: PMC8531997
- DOI: 10.1001/jamanetworkopen.2021.30479
Racial and Ethnic Disparities in Rates of COVID-19-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death in the United States From March 2020 to February 2021
Abstract
Importance: Racial and ethnic minority groups are disproportionately affected by COVID-19.
Objectives: To evaluate whether rates of severe COVID-19, defined as hospitalization, intensive care unit (ICU) admission, or in-hospital death, are higher among racial and ethnic minority groups compared with non-Hispanic White persons.
Design, setting, and participants: This cross-sectional study included 99 counties within 14 US states participating in the COVID-19-Associated Hospitalization Surveillance Network. Participants were persons of all ages hospitalized with COVID-19 from March 1, 2020, to February 28, 2021.
Exposures: Laboratory-confirmed COVID-19-associated hospitalization, defined as a positive SARS-CoV-2 test within 14 days prior to or during hospitalization.
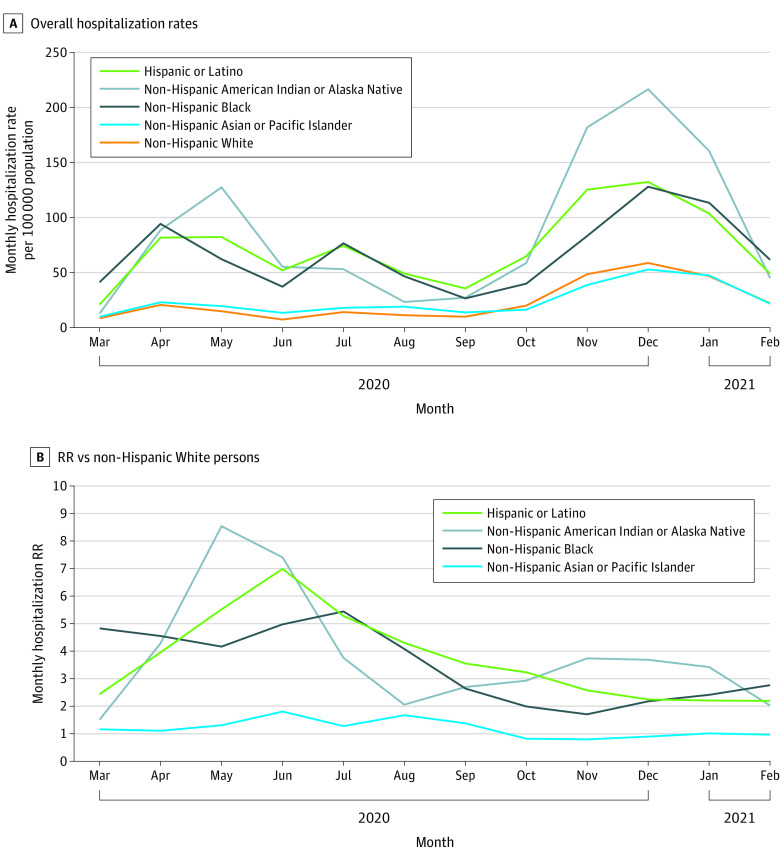
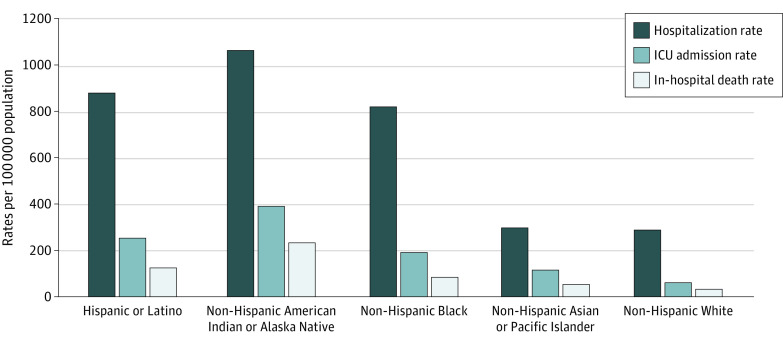
Main outcomes and measures: Cumulative age-adjusted rates (per 100 000 population) of hospitalization, ICU admission, and death by race and ethnicity. Rate ratios (RR) were calculated for each racial and ethnic group compared with White persons.
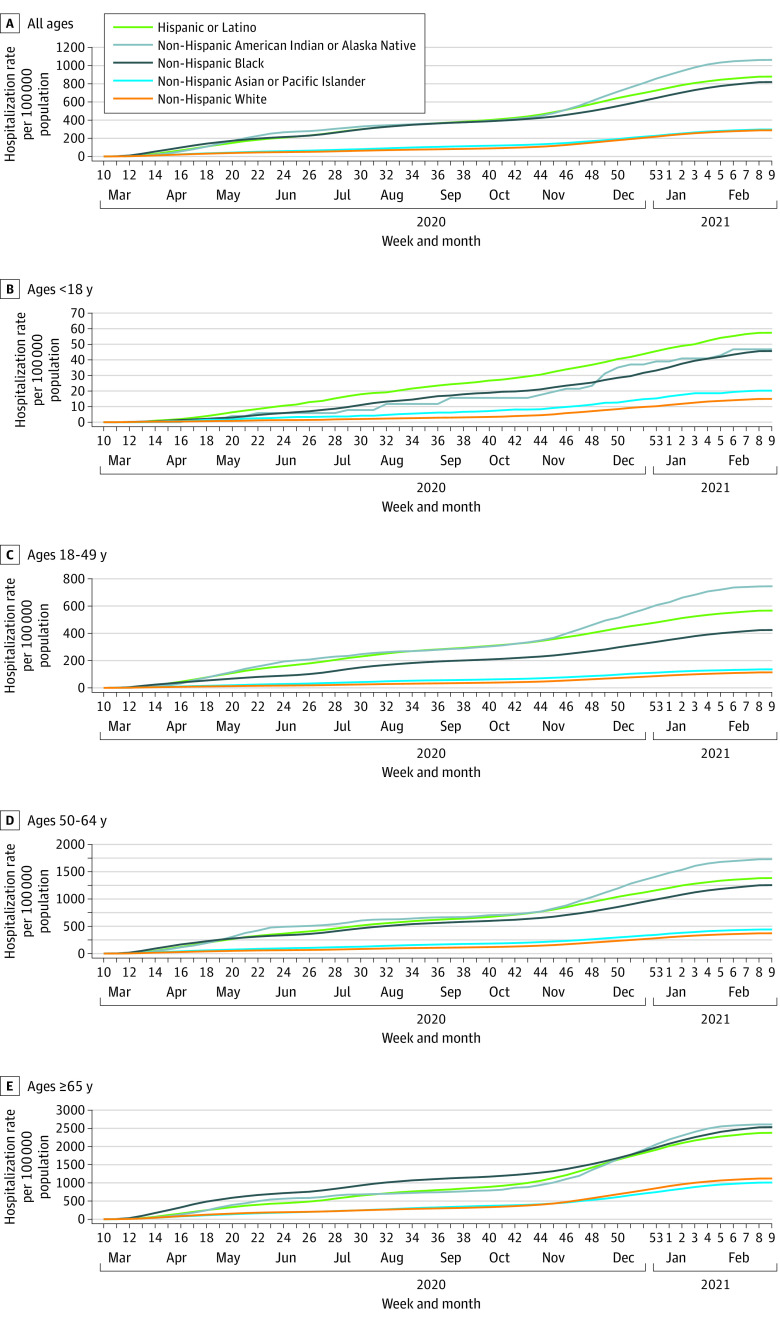
Results: Among 153 692 patients with COVID-19-associated hospitalizations, 143 342 (93.3%) with information on race and ethnicity were included in the analysis. Of these, 105 421 (73.5%) were 50 years or older, 72 159 (50.3%) were male, 28 762 (20.1%) were Hispanic or Latino, 2056 (1.4%) were non-Hispanic American Indian or Alaska Native, 7737 (5.4%) were non-Hispanic Asian or Pacific Islander, 40 806 (28.5%) were non-Hispanic Black, and 63 981 (44.6%) were White. Compared with White persons, American Indian or Alaska Native, Latino, Black, and Asian or Pacific Islander persons were more likely to have higher cumulative age-adjusted rates of hospitalization, ICU admission, and death as follows: American Indian or Alaska Native (hospitalization: RR, 3.70; 95% CI, 3.54-3.87; ICU admission: RR, 6.49; 95% CI, 6.01-7.01; death: RR, 7.19; 95% CI, 6.47-7.99); Latino (hospitalization: RR, 3.06; 95% CI, 3.01-3.10; ICU admission: RR, 4.20; 95% CI, 4.08-4.33; death: RR, 3.85; 95% CI, 3.68-4.01); Black (hospitalization: RR, 2.85; 95% CI, 2.81-2.89; ICU admission: RR, 3.17; 95% CI, 3.09-3.26; death: RR, 2.58; 95% CI, 2.48-2.69); and Asian or Pacific Islander (hospitalization: RR, 1.03; 95% CI, 1.01-1.06; ICU admission: RR, 1.91; 95% CI, 1.83-1.98; death: RR, 1.64; 95% CI, 1.55-1.74).
Conclusions and relevance: In this cross-sectional analysis, American Indian or Alaska Native, Latino, Black, and Asian or Pacific Islander persons were more likely than White persons to have a COVID-19-associated hospitalization, ICU admission, or in-hospital death during the first year of the US COVID-19 pandemic. Equitable access to COVID-19 preventive measures, including vaccination, is needed to minimize the gap in racial and ethnic disparities of severe COVID-19.
Conflict of interest statement
Figures
References
-
- US Centers for Disease Control and Prevention . COVID-19 racial and ethnic health disparities. CDC. Updated December 10, 2020. Accessed May 25, 2021. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/racial...
-
- Kim L, Garg S, O’Halloran A, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US Coronavirus Disease 2019 (COVID-19)–Associated Hospitalization Surveillance Network (COVID-NET). Clin Infect Dis. 2021;72(9):e206-e214. doi: 10.1093/cid/ciaa1012 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
