

Efficacy and Safety of a Fixed-Dose Clindamycin Phosphate 1.2%, Benzoyl Peroxide 3.1%, and Adapalene 0.15% Gel for Moderate-to-Severe Acne: A Randomized Phase II Study of the First Triple-Combination Drug
- PMID: 34674160
- PMCID: PMC8776677
- DOI: 10.1007/s40257-021-00650-3
Efficacy and Safety of a Fixed-Dose Clindamycin Phosphate 1.2%, Benzoyl Peroxide 3.1%, and Adapalene 0.15% Gel for Moderate-to-Severe Acne: A Randomized Phase II Study of the First Triple-Combination Drug
Abstract
Background: A three-pronged approach to acne treatment-combining an antibiotic, antibacterial, and retinoid-could provide greater efficacy and tolerability than single or dyad treatments, while potentially improving patient compliance and reducing antibiotic resistance.
Objectives: We aimed to evaluate the efficacy and safety of triple-combination, fixed-dose topical clindamycin phosphate 1.2%/benzoyl peroxide (BPO) 3.1%/adapalene 0.15% (IDP-126) gel for the treatment of acne.
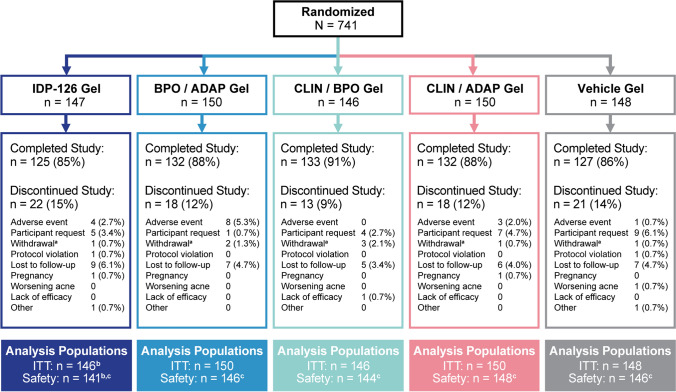
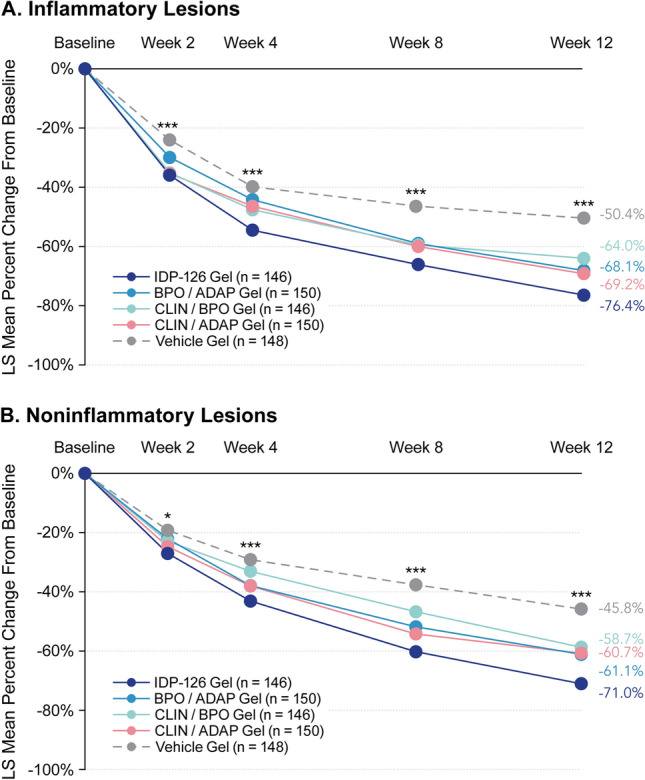
Methods: In a phase II, double-blind, multicenter, randomized, 12-week study, eligible participants aged ≥ 9 years with moderate-to-severe acne were equally randomized to once-daily IDP-126, vehicle, or one of three component dyad gels: BPO/adapalene; clindamycin phosphate/BPO; or clindamycin phosphate/adapalene. Coprimary endpoints were treatment success at week 12 (participants achieving a ≥ 2-grade reduction from baseline in Evaluator's Global Severity Score and clear/almost clear skin) and least-squares mean absolute changes from baseline in inflammatory and noninflammatory lesion counts to week 12. Treatment-emergent adverse events and cutaneous safety/tolerability were also assessed.
Results: A total of 741 participants were enrolled. At week 12, 52.5% of participants achieved treatment success with IDP-126 vs vehicle (8.1%) and dyads (range 27.8-30.5%; P ≤ 0.001, all). IDP-126 also provided significantly greater absolute reductions in inflammatory (29.9) and noninflammatory (35.5) lesions compared with vehicle or dyads (range inflammatory, 19.6-26.8; noninflammatory, 21.8-30.0; P < 0.05, all), corresponding to > 70% reductions with IDP-126. IDP-126 was well tolerated, with most treatment-emergent adverse events of mild-to-moderate severity.
Conclusions: Once-daily treatment with the novel fixed-dose triple-combination clindamycin phosphate 1.2%/BPO 3.1%/adapalene 0.15% gel demonstrated superior efficacy to vehicle and all three dyad component gels, and was well tolerated over 12 weeks in pediatric, adolescent, and adult participants with moderate-to-severe acne.
Clinical trial registration: ClinicalTrials.gov identifier NCT03170388 (registered 31 May, 2017).
© 2021. The Author(s).
Conflict of interest statement
Linda Stein Gold has served as an investigator/consultant or speaker for Ortho Dermatologics, LEO Pharma, Dermavant, Incyte, Novartis, AbbVie, Pfizer, Sun Pharma, UCB, Arcutis, and Lilly. Hilary Baldwin has served as an advisor or investigator and on speakers’ bureaus for Almirall, Cassiopea, Foamix, Galderma, Ortho Dermatologics, Sol Gel, and Sun Pharma. Leon H. Kircik has acted as an investigator, advisor, speaker, and consultant for Ortho Dermatologics. Jonathan S. Weiss is a consultant, speaker, advisor, and/or researcher for AbbVie, Ortho Dermatologics, Janssen Biotech, Dermira, Almirall, Brickell Biotech, DermTech, and Scynexis. David M. Pariser has served as a consultant to Atacama Therapeutics, Bickel Biotechnology, Biofrontera AG, Celgene, Dermira, LEO Pharma, Regeneron, Sanofi, TDM SurgiTech, TheraVida, and Ortho Dermatologics; an investigator for Abbott Laboratories, Almirall, Amgen, AOBiome, Asana Biosciences, Bickel Biotechnology, Celgene, Dermavant, Dermira, Eli Lilly, LEO Pharma, Menlo Therapeutics, Merck & Co., Novartis, Novo Nordisk A/S, Ortho Dermatologics, Pfizer, Regeneron, and Stiefel; on the advisory board for Pfizer; and on the data monitoring board for BMS. Valerie Callender has served as an investigator, consultant, or speaker for AbbVie, Galderma, L’Oréal, Ortho Dermatologics, and Vyne. Edward Lain has nothing to disclose. Michael Gold has acted as an investigator, advisor, speaker, and consultant for Ortho Dermatologics. Kenneth Beer has received funding from Allergan, Galderma, Evolus, and Revance. Zoe Draelos received research funding from Ortho Dermatologics. Neil Sadick has served on advisory boards, as a consultant, investigator, speaker, and/or other and has received honoraria and/or grants/research funding from Almirall, Actavis, Allergan, Anacor Pharmaceuticals, Auxilium Pharmaceuticals, Bausch Health, Bayer, Biorasi, BTG, Carma Laboratories, Cassiopea, Celgene Corporation, Cutera, Cynosure, DUSA Pharmaceuticals, Eclipse Medical, Eli Lilly and Company, Endo International, EndyMed Medical, Ferndale Laboratories, Galderma, Gerson Lehrman Group, Hydropeptide, Merz Aesthetics, Neostrata, Novartis, Nutraceutical Wellness, Palomar Medical Technologies, Prescriber’s Choice, Regeneron, Roche Laboratories, Samumed, Solta Medical, Storz Medical AG, Suneva Medical, Vanda Pharmaceuticals, and Venus Concept. Radhakrishnan Pillai and Varsha Bhatt are employees of Bausch Health US, LLC and may hold stock and/or stock options in its parent company. Emil A. Tanghetti has served as a speaker for Novartis, Ortho Dermatologics, Sun Pharma, Lilly, Galderma, AbbVie, and Dermira; served as a consultant in clinical studies for Hologic, Ortho Dermatologics, and Galderma; and is a stockholder for Accure.
Figures
References
-
- Del Rosso JQ, Schmidt NF. A review of the anti-inflammatory properties of clindamycin in the treatment of acne vulgaris. Cutis. 2010;85(1):15–24. - PubMed
-
- Yentzer BA, Ade RA, Fountain JM, Clark AR, Taylor SL, Fleischer AB, Jr, et al. Simplifying regimens promotes greater adherence and outcomes with topical acne medications: a randomized controlled trial. Cutis. 2010;86(2):103–108. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
