

Biomechanical analysis of subcondylar fracture fixation using miniplates at different positions and of different lengths
- PMID: 34674692
- PMCID: PMC8532336
- DOI: 10.1186/s12903-021-01905-5
Biomechanical analysis of subcondylar fracture fixation using miniplates at different positions and of different lengths
Abstract
Background: Many types of titanium plates were used to treat subcondylar fracture clinically. However, the efficacy of fixation in different implant positions and lengths of the bone plate has not been thoroughly investigated. Therefore, the primary purpose of this study was to use finite element analysis (FEA) to analyze the biomechanical effects of subcondylar fracture fixation with miniplates at different positions and lengths so that clinicians were able to find a better strategy of fixation to improve the efficacy and outcome of treatment.
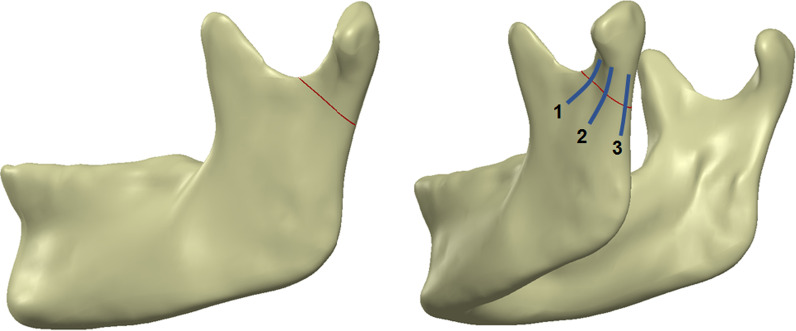
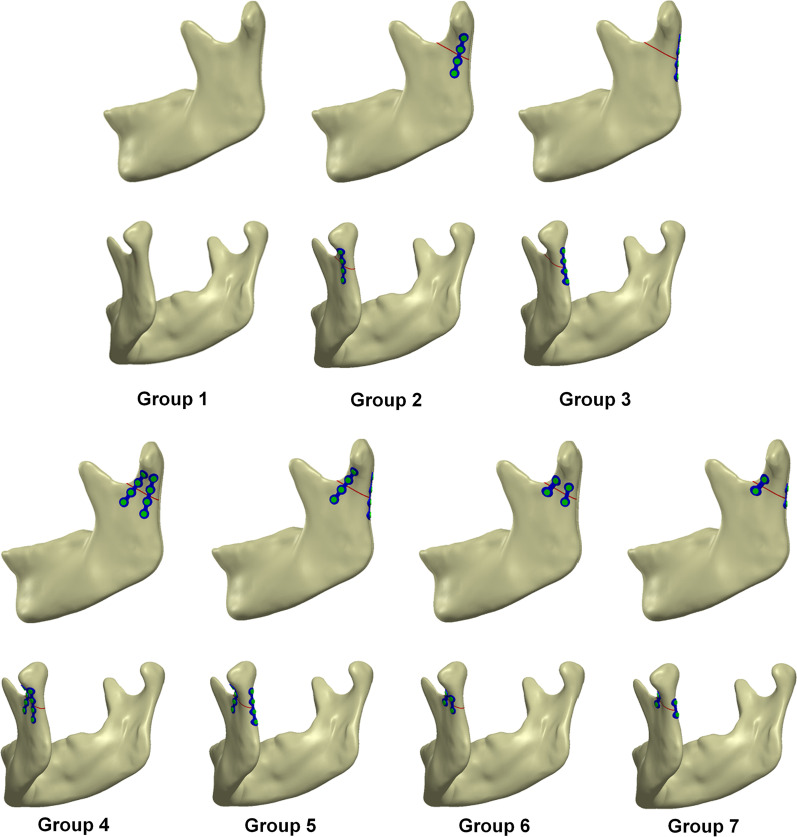
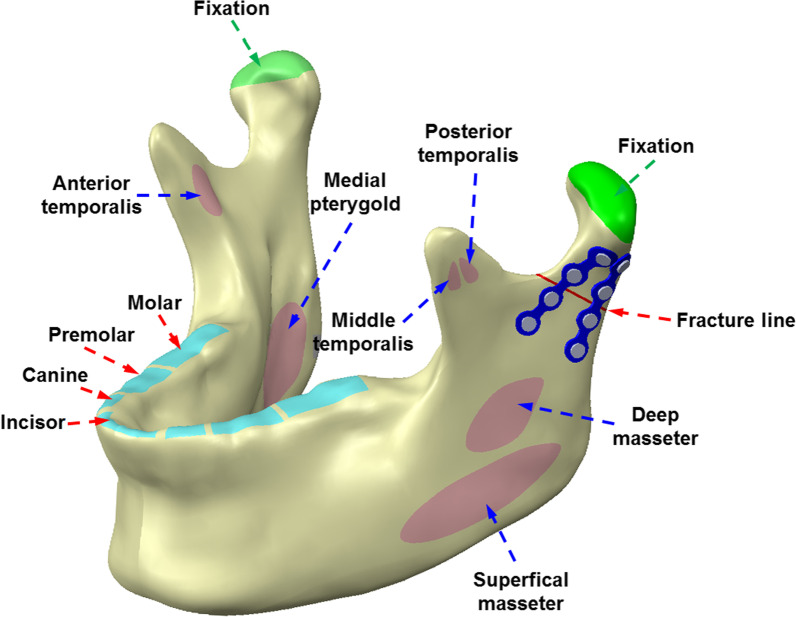
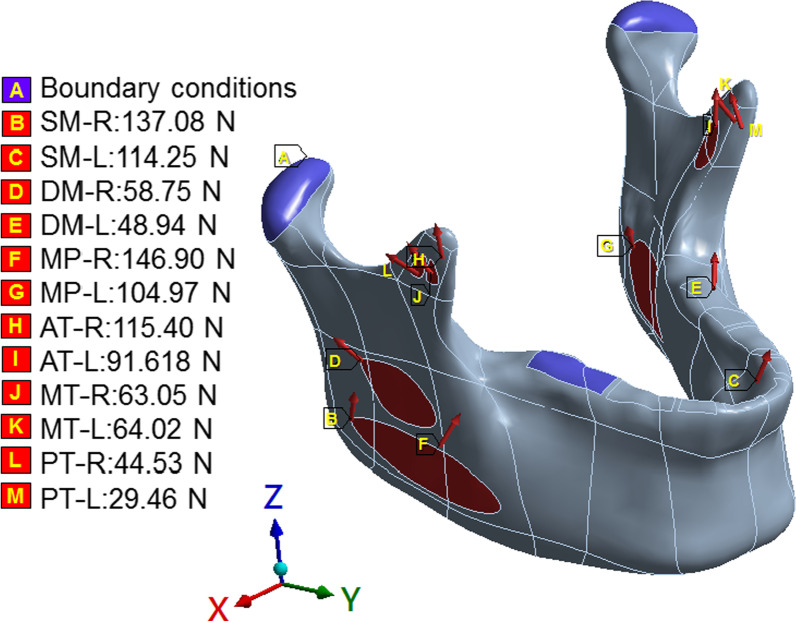
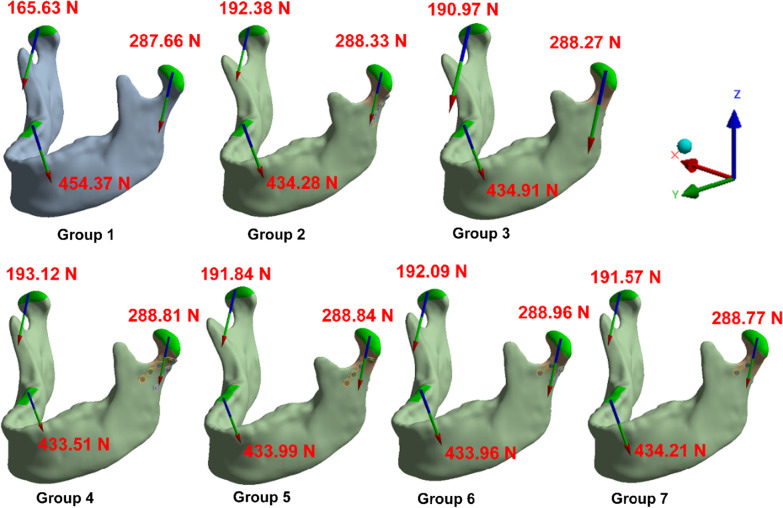
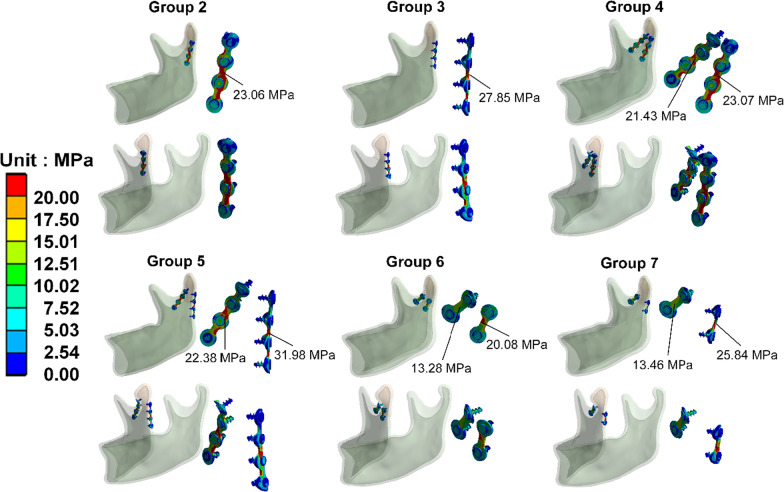
Methods: The CAD software was used to combine the mandible, miniplate, and screw to create seven different FEA computer models. These models with subcondylar fracture were fixed with miniplates at different positions and of different lengths. The right unilateral molar clench occlusal mode was applied. The observational indicators were the reaction force at the temporomandibular joint, von Mises stress of the mandibular bone, miniplate and screw, and the sliding distance on the oblique surface of the fracture site at the mandibular condyle.
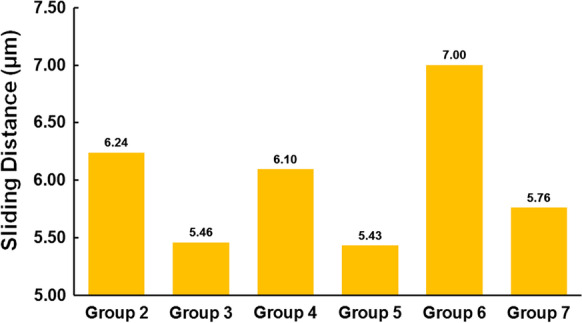
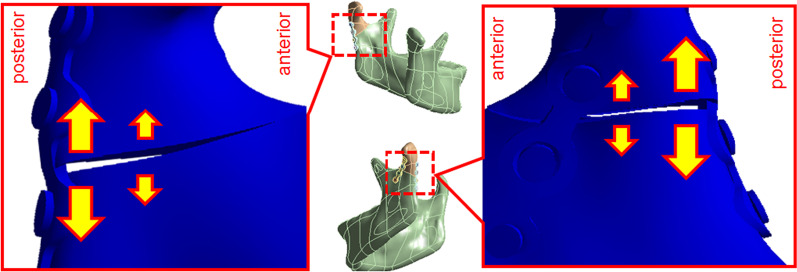
Results: The results showed the efficacy of fixation was better when two miniplates were used comparing to only one miniplates. Moreover, using longer miniplates for fixation had better results than the short one. Furthermore, fixing miniplates at the posterior portion of subcondylar region would have a better fixation efficacy and less sliding distance (5.46-5.76 μm) than fixing at the anterolateral surface of subcondylar region (6.10-7.00 μm).
Conclusion: Miniplate fixation, which was placed closer to the posterior margin, could effectively reduce the amount of sliding distance in the fracture site, thereby achieving greater stability. Furthermore, fixation efficiency was improved when an additional miniplate was placed at the anterior margin. Our study suggested that the placement of miniplates at the posterior surface and the additional plate could effectively improve stability.
Keywords: Miniplates; Open reduction and internal fixation; Subcondylar fracture.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Bormann K-H, Wild S, Gellrich N-C, Kokemüller H, Stühmer C, Schmelzeisen R, Schön R. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg. 2009;67:1251–1255. doi: 10.1016/j.joms.2008.09.022. - DOI - PubMed
-
- Asim MA, Ibrahim MW, Javed MU, Zahra R, Qayyum MU. Functional outcomes of open versus closed treatment of unilateral mandibular condylar fractures. J Ayub Med Coll Abbottabad. 2019;31:67–71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
