

A case of ectopic pancreas of the stomach accompanied by intraductal papillary mucinous neoplasm with GNAS mutation
- PMID: 34674710
- PMCID: PMC8529847
- DOI: 10.1186/s12957-021-02424-x
A case of ectopic pancreas of the stomach accompanied by intraductal papillary mucinous neoplasm with GNAS mutation
Abstract
Background: Ectopic pancreas is basically a benign disease and is not always necessary to be removed. However, all types of neoplasms occurring in the normal pancreas such as ductal adenocarcinomas and intraductal papillary mucinous neoplasms (IPMNs) may develop even within ectopic pancreas. We recently encountered an extremely rare case of ectopic pancreas in the gastric antrum associated with IPMN possessing a GNAS mutation.
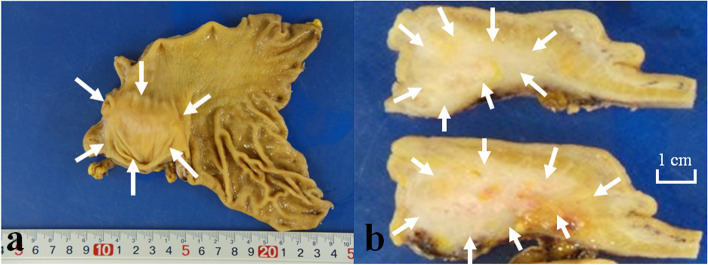
Case presentation: A 71-year-old Japanese woman complained of epigastric pain. Computed tomography and upper gastrointestinal endoscopy showed an intramural cystic mass in the antrum of the stomach. Endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) biopsy did not give a definitive diagnosis, and the patient underwent resection of the lesion. Histology of the resected specimen showed that the gastric intramural lesion was ectopic pancreas. Moreover, the lesion contained dilated duct components with tubulo-villous epithelial proliferation consistent with pancreatic IPMN. Since the covering epithelial cells had highly atypical nuclei, the lesion was diagnosed as IPMN with high grade dysplasia. Immunohistochemistry showed that the IPMN component showed to be MUC2-, MUC5AC-, and CDX2-positive but MUC1- and MUC6-negative. Mutational analyses using genomic DNA revealed that the IPMN component had a mutation of GNAS at exon 8 (Arg201Cys).
Conclusion: We finally diagnosed this case as gastric ectopic pancreas accompanied by intestinal type IPMN with high grade dysplasia possessing GNAS mutation. Although there were 17 cases of ectopic pancreas with IPMN including 6 cases of gastric ones reported in the English literature, this is the first case of ectopic pancreas with IPMN which was proved to have GNAS mutation. Intimate preoperative examinations including imaging analyses and EUS-FNA biopsy/cytology are recommended to decide whether the lesion has to be resected or not even if they are not effective for getting the right diagnosis.
Keywords: Ectopic pancreas; GNAS mutation; Heterotopic pancreas; IPMN; Intraductal papillary mucinous neoplasm; Pancreatic heterotopia.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Intraductal papillary mucinous neoplasms of the pancreas with distinct pancreatic ductal adenocarcinomas are frequently of gastric subtype.Ann Surg. 2013 Jul;258(1):141-51. doi: 10.1097/SLA.0b013e31828cd008. Ann Surg. 2013. PMID: 23532108
-
Clinical assessment of the GNAS mutation status in patients with intraductal papillary mucinous neoplasm of the pancreas.Surg Today. 2019 Nov;49(11):887-893. doi: 10.1007/s00595-019-01797-7. Epub 2019 Mar 16. Surg Today. 2019. PMID: 30879148 Review.
-
Value of adding GNAS testing to pancreatic cyst fluid KRAS and carcinoembryonic antigen analysis for the diagnosis of intraductal papillary mucinous neoplasms.Dig Endosc. 2017 Jan;29(1):111-117. doi: 10.1111/den.12710. Epub 2016 Oct 4. Dig Endosc. 2017. PMID: 27514845
-
Clinical significance of GNAS mutation in intraductal papillary mucinous neoplasm of the pancreas with concomitant pancreatic ductal adenocarcinoma.Pancreas. 2015 Mar;44(2):311-20. doi: 10.1097/MPA.0000000000000258. Pancreas. 2015. PMID: 25479586
-
Intraductal Papillary Mucinous Neoplasm Arising from Heterotopic Pancreas in Stomach: A Case Report and Review of Literature.Int J Surg Pathol. 2023 Aug;31(5):708-713. doi: 10.1177/10668969221117990. Epub 2022 Aug 9. Int J Surg Pathol. 2023. PMID: 35946106 Review.
Cited by
-
Laparoscopic resection and endoscopic submucosal dissection for treating gastric ectopic pancreas.World J Gastrointest Surg. 2023 Dec 27;15(12):2799-2808. doi: 10.4240/wjgs.v15.i12.2799. World J Gastrointest Surg. 2023. PMID: 38222013 Free PMC article.
-
Adenocarcinoma developing from gastric heterotopic pancreas: a case report and short review.Front Surg. 2024 May 9;11:1274389. doi: 10.3389/fsurg.2024.1274389. eCollection 2024. Front Surg. 2024. PMID: 38783861 Free PMC article.
References
-
- Bastuk O, Hong SM, Esposito I, Klöppel G, Fukushima N, Maitra A, et al. Digestive system WHO classification of tumours. 5. 2019. Pancreatic intraductal papillary mucinous neoplasm; pp. 310–314.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
