

Modification effect of ideal cardiovascular health metrics on genetic association with incident heart failure in the China Kadoorie Biobank and the UK Biobank
- PMID: 34674714
- PMCID: PMC8532287
- DOI: 10.1186/s12916-021-02122-1
Modification effect of ideal cardiovascular health metrics on genetic association with incident heart failure in the China Kadoorie Biobank and the UK Biobank
Abstract
Background: Both genetic and cardiovascular factors contribute to the risk of developing heart failure (HF), but whether idea cardiovascular health metrics (ICVHMs) offset the genetic association with incident HF remains unclear.
Objectives: To investigate the genetic association with incident HF as well as the modification effect of ICVHMs on such genetic association in Chinese and British populations.
Methods: An ICVHMs based on smoking, drinking, physical activity, diets, body mass index, waist circumference, blood pressure, blood glucose, and blood lipids, and a polygenic risk score (PRS) for HF were constructed in the China Kadoorie Biobank (CKB) of 96,014 participants and UK Biobank (UKB) of 335,782 participants which were free from HF and severe chronic diseases at baseline.
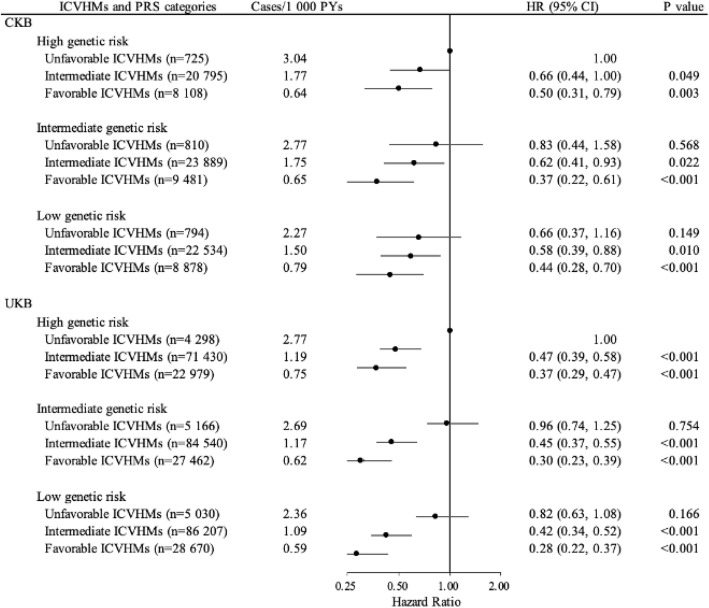
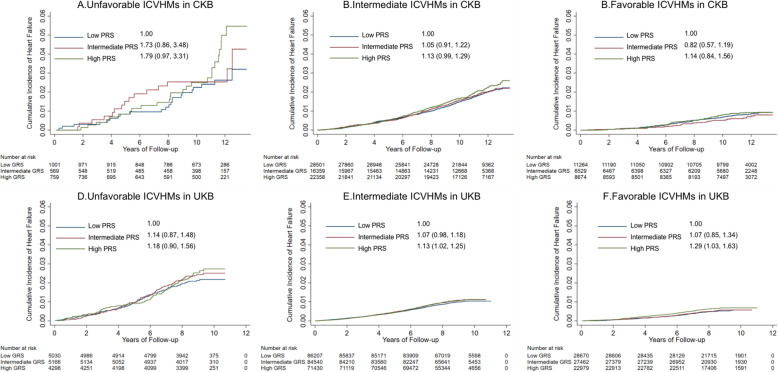
Results: During the median follow-up of 11.38 and 8.73 years, 1451 and 3169 incident HF events were documented in CKB and UKB, respectively. HF risk increased monotonically with the increase of PRS per standard deviation (CKB: hazard ratio [HR], 1.19; 95% confidence interval [CI], 1.07, 1.32; UKB: 1.07; 1.03, 1.11; P for trend < 0.001). Each point increase in ICVHMs was associated with 15% and 20% lower risk of incident HF in CKB (0.85; 0.81, 0.90) and UKB (0.80; 0.77, 0.82), respectively. Compared with unfavorable ICVHMs, favorable ICVHMs was associated with a lower HF risk, with 0.71 (0.44, 1.15), 0.41 (0.22, 0.77), and 0.48 (0.30, 0.77) in the low, intermediate, and high genetic risk in CKB and 0.34 (0.26, 0.44), 0.32 (0.25, 0.41), and 0.37 (0.28, 0.47) in UKB (P for multiplicative interaction > 0.05). Participants with low genetic risk and favorable ICVHMs, as compared with high genetic risk and unfavorable ICVHMs, had 56~72% lower risk of HF (CKB 0.44; 0.28, 0.70; UKB 0.28; 0.22, 0.37). No additive interaction between PRS and ICVHMs was observed (relative excess risk due to interaction was 0.05 [-0.22, 0.33] in CKB and 0.04 [-0.14, 0.22] in UKB).
Conclusions: In CKB and UKB, genetic risk and ICVHMs were independently associated with the risk of incident HF, which suggested that adherence to favorable cardiovascular health status was associated with a lower HF risk among participants with all gradients of genetic risk.
Keywords: Genetic risk; Heart failure; Ideal cardiovascular health metrics.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Importance of healthy lifestyle factors and ideal cardiovascular health metrics for risk of heart failure in Chinese adults.Int J Epidemiol. 2022 May 9;51(2):567-578. doi: 10.1093/ije/dyab236. Int J Epidemiol. 2022. PMID: 34931664
-
Ideal Cardiovascular Health Metrics and Major Cardiovascular Events in Patients With Prediabetes and Diabetes.JAMA Cardiol. 2019 Sep 1;4(9):874-883. doi: 10.1001/jamacardio.2019.2499. JAMA Cardiol. 2019. PMID: 31365039 Free PMC article.
-
Intakes of major food groups in China and UK: results from 100,000 adults in the China Kadoorie biobank and UK biobank.Eur J Nutr. 2023 Mar;62(2):819-832. doi: 10.1007/s00394-022-03031-6. Epub 2022 Oct 22. Eur J Nutr. 2023. PMID: 36271961 Free PMC article.
-
Association of Life's Essential 8 with incidence of heart failure modified by depressive symptoms: a prospective cohort study from UK Biobank.BMC Med. 2025 Mar 24;23(1):175. doi: 10.1186/s12916-025-04011-3. BMC Med. 2025. PMID: 40128779 Free PMC article.
-
An Opportunity for Prevention: Associations Between the Life's Essential 8 Score and Cardiovascular Incidence Using Prospective Data from UK Biobank.Curr Probl Cardiol. 2023 Apr;48(4):101540. doi: 10.1016/j.cpcardiol.2022.101540. Epub 2022 Dec 14. Curr Probl Cardiol. 2023. PMID: 36528209 Review.
Cited by
-
Lactation duration and ischemic heart disease among parous postmenopausal females from a prospective cohort study.Commun Med (Lond). 2025 Mar 25;5(1):86. doi: 10.1038/s43856-025-00806-w. Commun Med (Lond). 2025. PMID: 40128564 Free PMC article.
-
Physical Activity and All-Cause Mortality by Age in 4 Multinational Megacohorts.JAMA Netw Open. 2024 Nov 4;7(11):e2446802. doi: 10.1001/jamanetworkopen.2024.46802. JAMA Netw Open. 2024. PMID: 39570587 Free PMC article.
-
Association of Sleep Pattern and Genetic Susceptibility with Obstructive Sleep Apnea: A Prospective Analysis of the UK Biobank.Nat Sci Sleep. 2024 May 23;16:503-515. doi: 10.2147/NSS.S443721. eCollection 2024. Nat Sci Sleep. 2024. PMID: 38803507 Free PMC article.
-
Epidemiology and Burden of Heart Failure in Asia.JACC Asia. 2024 Mar 19;4(4):249-264. doi: 10.1016/j.jacasi.2024.01.013. eCollection 2024 Apr. JACC Asia. 2024. PMID: 38660101 Free PMC article. Review.
-
Choline Metabolites, Genetic Susceptibility, and Incident Heart Failure.JACC Adv. 2024 Dec 14;4(1):101445. doi: 10.1016/j.jacadv.2024.101445. eCollection 2025 Jan. JACC Adv. 2024. PMID: 39791104 Free PMC article.
References
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545-602. 10.1016/s0140-6736(16)31678-6. - PMC - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. ESC Heart Fail. 2016;18(8):891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
-
- Lindmark K, Boman K, Olofsson M, Törnblom M, Levine A, Castelo-Branco A, Schlienger R, Bruce Wirta S, Stålhammar J, Wikström G. Epidemiology of heart failure and trends in diagnostic work-up: a retrospective, population-based cohort study in Sweden. Clin Epidemiol. 2019;11:231–244. doi: 10.2147/clep.S170873. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- MC_U137686851/MRC_/Medical Research Council/United Kingdom
- 16896/CRUK_/Cancer Research UK/United Kingdom
- CH/1996001/9454/BHF_/British Heart Foundation/United Kingdom
- 212946/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- MC_UU_12026/2/MRC_/Medical Research Council/United Kingdom
- MC_PC_14135/MRC_/Medical Research Council/United Kingdom
- MC_UU_00017/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- MC_PC_13049/MRC_/Medical Research Council/United Kingdom
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- 29186/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
