

Anatomic Neuroimaging Characteristics of Posterior Fossa Type A Ependymoma Subgroups
- PMID: 34674998
- PMCID: PMC8805767
- DOI: 10.3174/ajnr.A7322
Anatomic Neuroimaging Characteristics of Posterior Fossa Type A Ependymoma Subgroups
Abstract
Background and purpose: Posterior fossa type A (PFA) ependymomas have 2 molecular subgroups (PFA-1 and PFA-2) and 9 subtypes. Gene expression profiling suggests that PFA-1 and PFA-2 tumors have distinct developmental origins at different rostrocaudal levels of the brainstem. We, therefore, tested the hypothesis that PFA-1 and PFA-2 ependymomas have different anatomic MR imaging characteristics at presentation.
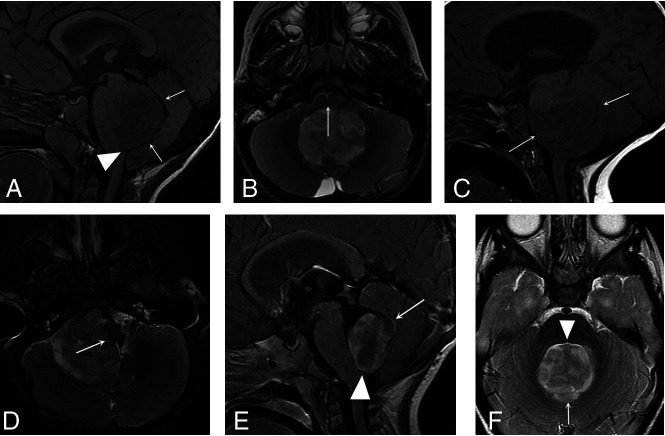
Materials and methods: Two neuroradiologists reviewed the preoperative MR imaging examinations of 122 patients with PFA ependymomas and identified several anatomic characteristics, including extension through the fourth ventricular foramina and encasement of major arteries and tumor type (midfloor, roof, or lateral). Deoxyribonucleic acid methylation profiling assigned ependymomas to PFA-1 or PFA-2. Information on PFA subtype from an earlier study was also available for a subset of tumors. Associations between imaging variables and subgroup or subtype were evaluated.
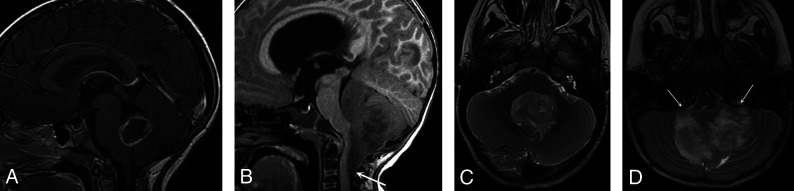
Results: No anatomic imaging variable was significantly associated with the PFA subgroup, but 5 PFA-2c subtype ependymomas in the cohort had a more circumscribed appearance and showed less tendency to extend through the fourth ventricular foramina or encase blood vessels, compared with other PFA subtypes.
Conclusions: PFA-1 and PFA-2 ependymomas did not have different anatomic MR imaging characteristics, and these results do not support the hypothesis that they have distinct anatomic origins. PFA-2c ependymomas appear to have a more anatomically circumscribed MR imaging appearance than the other PFA subtypes; however, this needs to be confirmed in a larger study.
© 2021 by American Journal of Neuroradiology.
Figures
Similar articles
-
Imaging features to distinguish posterior fossa ependymoma subgroups.Eur Radiol. 2024 Mar;34(3):1534-1544. doi: 10.1007/s00330-023-10182-5. Epub 2023 Sep 2. Eur Radiol. 2024. PMID: 37658900
-
Molecular heterogeneity and CXorf67 alterations in posterior fossa group A (PFA) ependymomas.Acta Neuropathol. 2018 Aug;136(2):211-226. doi: 10.1007/s00401-018-1877-0. Epub 2018 Jun 16. Acta Neuropathol. 2018. PMID: 29909548 Free PMC article.
-
TERT promoter mutation and chromosome 6 loss define a high-risk subtype of ependymoma evolving from posterior fossa subependymoma.Acta Neuropathol. 2021 Jun;141(6):959-970. doi: 10.1007/s00401-021-02300-8. Epub 2021 Mar 23. Acta Neuropathol. 2021. PMID: 33755803 Free PMC article.
-
Recurrent pediatric infratentorial ependymomas: a systematic review and meta-analysis on outcomes and molecular classification.J Neurosurg Pediatr. 2022 Nov 25;31(2):132-142. doi: 10.3171/2022.10.PEDS22154. Print 2023 Feb 1. J Neurosurg Pediatr. 2022. PMID: 36433871
-
EZHIP: a new piece of the puzzle towards understanding pediatric posterior fossa ependymoma.Acta Neuropathol. 2022 Jan;143(1):1-13. doi: 10.1007/s00401-021-02382-4. Epub 2021 Nov 11. Acta Neuropathol. 2022. PMID: 34762160 Free PMC article. Review.
Cited by
-
Ependymal Tumors: Overview of the Recent World Health Organization Histopathologic and Genetic Updates with an Imaging Characteristic.AJNR Am J Neuroradiol. 2024 Nov 7;45(11):1624-1634. doi: 10.3174/ajnr.A8237. AJNR Am J Neuroradiol. 2024. PMID: 38844368 Review.
-
Arterial Spin-Labeling Perfusion Lightbulb Sign: An Imaging Biomarker of Pediatric Posterior Fossa Hemangioblastoma.AJNR Am J Neuroradiol. 2024 Nov 7;45(11):1784-1790. doi: 10.3174/ajnr.A8391. AJNR Am J Neuroradiol. 2024. PMID: 38914433
-
Newly Recognized CNS Tumors in the 2021 World Health Organization Classification: Imaging Overview with Histopathologic and Genetic Correlation.AJNR Am J Neuroradiol. 2023 Apr;44(4):367-380. doi: 10.3174/ajnr.A7827. Epub 2023 Mar 30. AJNR Am J Neuroradiol. 2023. PMID: 36997287 Free PMC article. Review.
-
Lateral-type posterior fossa ependymomas in pediatric patients: a national collaborative study.Childs Nerv Syst. 2024 Feb;40(2):407-416. doi: 10.1007/s00381-023-06194-7. Epub 2023 Oct 27. Childs Nerv Syst. 2024. PMID: 37889277
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources