

Temporal trends in pulmonary arterial hypertension: results from the COMPERA registry
- PMID: 34675047
- PMCID: PMC9160392
- DOI: 10.1183/13993003.02024-2021
Temporal trends in pulmonary arterial hypertension: results from the COMPERA registry
Abstract
Background: Since 2015, the European pulmonary hypertension guidelines recommend the use of combination therapy in most patients with pulmonary arterial hypertension (PAH). However, it is unclear to what extent this treatment strategy is adopted in clinical practice and if it is associated with improved long-term survival.
Methods: We analysed data from COMPERA, a large European pulmonary hypertension registry, to assess temporal trends in the use of combination therapy and survival of patients with newly diagnosed PAH between 2010 and 2019. For survival analyses, we looked at annualised data and at cumulated data comparing the periods 2010-2014 and 2015-2019.
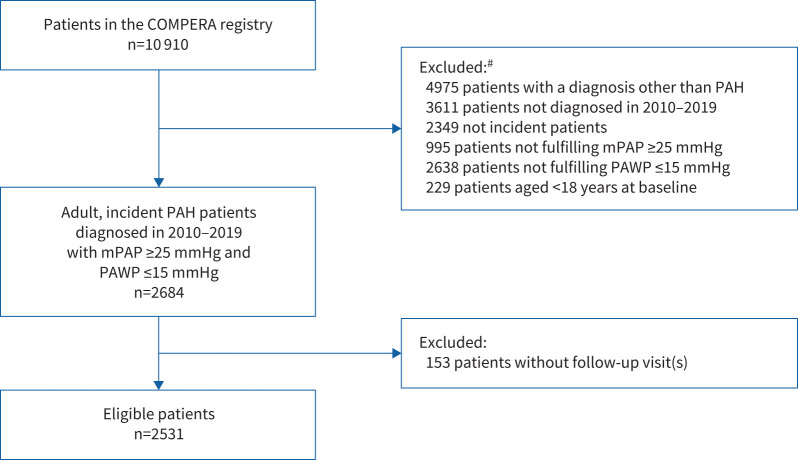
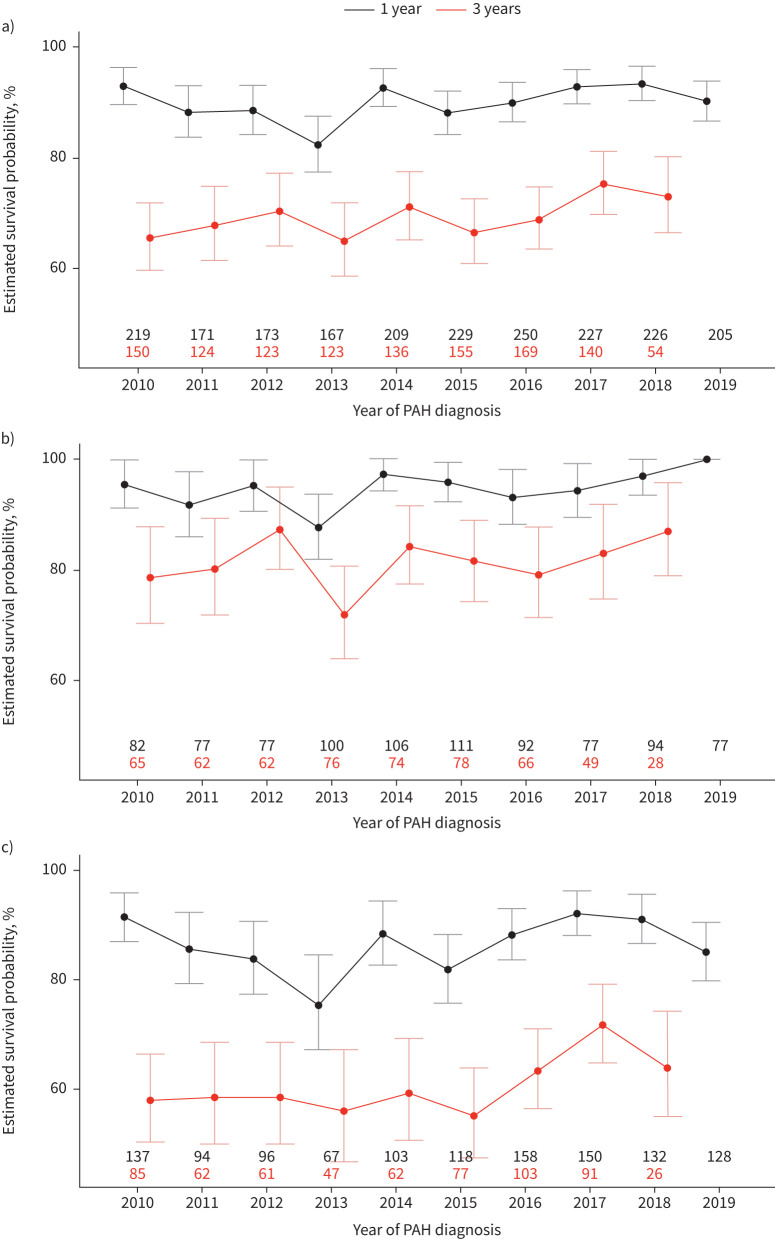
Results: A total of 2531 patients were included. The use of early combination therapy (within 3 months after diagnosis) increased from 10.0% in patients diagnosed with PAH in 2010 to 25.0% in patients diagnosed with PAH in 2019. The proportion of patients receiving combination therapy 1 year after diagnosis increased from 27.7% to 46.3%. When comparing the 2010-2014 and 2015-2019 periods, 1-year survival estimates were similar (89.0% (95% CI 87.2-90.9%) and 90.8% (95% CI 89.3-92.4%), respectively), whereas there was a slight but nonsignificant improvement in 3-year survival estimates (67.8% (95% CI 65.0-70.8%) and 70.5% (95% CI 67.8-73.4%), respectively).
Conclusions: The use of combination therapy increased from 2010 to 2019, but most patients still received monotherapy. Survival rates at 1 year after diagnosis did not change over time. Future studies need to determine if the observed trend suggesting improved 3-year survival rates can be confirmed.
Copyright ©The authors 2022.
Conflict of interest statement
Conflicts of interest: M.M. Hoeper has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GlaxoSmithKline, Janssen, MSD and Pfizer. Conflicts of interest: C. Pausch has no disclosures. Conflicts of interest: E. Grünig has received fees for lectures and/or consultations from Actelion, Bayer, GlaxoSmithKline, Janssen, MSD, Pfizer and United Therapeutics. Conflicts of interest: G. Staehler has received honoraria for lectures and/or consultancy for Actelion, Bayer, GlaxoSmithKline, Novartis and Pfizer. Conflicts of interest: D. Huscher has received consulting fees from Actelion. Conflicts of interest: D. Pittrow has received fees for consultations from Actelion, Amgen, Aspen, Bayer, Biogen, Boehringer Ingelheim, Daiichi Sankyo, Sanofi, Takeda and Viatris. Conflicts of interest: K.M. Olsson has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GlaxoSmithKline, Janssen, MSD, Pfizer and United Therapeutics. Conflicts of interest: C.D. Vizza has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GlaxoSmithKline, Janssen, MSD, Pfizer and United Therapeutics. Conflicts of interest: H. Gall reports personal fees from Actelion, AstraZeneca, Bayer, BMS, GlaxoSmithKline, Janssen-Cilag, Lilly, MSD, Novartis, OMT, Pfizer and United Therapeutics. Conflicts of interest: O. Distler has/had consultancy relationship and/or has received research funding from 4D Science, Actelion, Active Biotec, Bayer, Biogen Idec, Boehringer Ingelheim Pharma, BMS, ChemoAb, EpiPharm, Ergonex, EspeRare Foundation, GlaxoSmithKline, Genentech/Roche, Inventiva, Janssen, Lilly, medac, MedImmune, Mitsubishi Tanabe, Pharmacyclics, Pfizer, Sanofi, Serodapharm and Sinoxa, in the area of potential treatments of scleroderma and its complications including PAH; in addition, the author has a patent “mir-29 for the treatment of systemic sclerosis” licensed. Conflicts of interest: C. Opitz has received speaker fees and honoraria for consultations from Actelion, Bayer, GlaxoSmithKline, Lilly, Novartis and Pfizer. Conflicts of interest: J.S.R. Gibbs has received fees for lectures and/or consultations from Acceleron, Actelion, Aerovate, Bayer, Complexia, Janssen, MSD, Pfizer and United Therapeutics. Conflicts of interest: M. Delcroix reports research grants from Actelion/J&J, speaker and consultant fees from Bayer, MSD, Acceleron, AOP and Daiichi Sankyo, outside the submitted work; and is holder of the Janssen Chair for Pulmonary Hypertension at the KU Leuven. Conflicts of interest: H.A. Ghofrani has received honoraria for consultations and/or speaking at conferences from Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Lilly and Novartis; is member of advisory boards for Acceleron, Bayer HealthCare AG, Pfizer, GlaxoSmithKline, Actelion, Lilly, Merck, Encysive and Ergonex; and has also received governmental grants from the German Research Foundation (DFG), Excellence Cluster Cardiopulmonary Research (ECCPS), State Government of Hessen (LOEWE) and the German Ministry for Education and Research (BMBF). Conflicts of interest: S. Rosenkranz has received fees for lectures and/or consultations from Abbott, Acceleron, Actelion, Bayer, BMS, Gilead, GlaxoSmithKline, Janssen, MSD, Novartis, Pfizer, United Therapeutics and Vifor; research grants to institution from AstraZeneca, Actelion, Bayer Janssen and Novartis. Conflicts of interest: D-H. Park has nothing to disclose. Conflicts of interest: R. Ewert has received speaker fees and honoraria for consultations from Actelion, Bayer, GlaxoSmithKline, Janssen, Lilly, MSD, Novartis, Pfizer and United Therapeutics. Conflicts of interest: H. Kaemmerer has received honoraria for lectures and/or consultancy from Actelion, BMS and Janssen. Conflicts of interest: T.J. Lange has received speaker fees and honoraria for consultation from Acceleron, Actelion, Bayer, GlaxoSmithKline, Janssen-Cilag, MSD, Pfizer and United Therapeutics. Conflicts of interest: H-J. Kabitz has received fees from Löwenstein Medical, Weinmann, Philips Respironics, ResMed, Vivisol, Sapio Life and Sanofi-Genzyme. Conflicts of interest: D. Skowasch received fees for lectures and/or consulting and/or research support to institution from Actelion, Bayer, GlaxoSmithKline, Janssen, MSD and Pfizer. Conflicts of interest: A. Skride reports no conflicts of interest. Conflicts of interest: M. Claussen reports honoraria for lectures from Boehringer Ingelheim Pharma GmbH and Roche Pharma, and for serving on advisory boards from Boehringer Ingelheim. Conflicts of interest: J. Behr received grants from Actelion, Bayer, Biogen, Boehringer Ingelheim, Galapagos, Novartis, Roche and Sanofi/Genzyme. Conflicts of interest: K. Milger has received fees from Actelion, AstraZeneca, GlaxoSmithKline, Janssen, MSD, Novartis and Sanofi-Aventis. Conflicts of interest: M. Halank has received speaker fees and honoraria for consultations from Acceleron, Actelion, AstraZeneca, Bayer, BerlinChemie, GlaxoSmithKline, Janssen and Novartis. Conflicts of interest: H. Wilkens received personal fees from Actelion, Bayer, Biotest, Boehringer, GlaxoSmithKline, Janssen, Pfizer and Roche. Conflicts of interest: H-J. Seyfarth has received speaker fees and honoraria for consultations from Actelion, Bayer, GlaxoSmithKline, Janssen and MSD. Conflicts of interest: M. Held has received speaker fees and honoraria for consultations from Actelion, Bayer, Boehringer Ingelheim Pharma, GlaxoSmithKline, Janssen, MSD, Novartis, Pfizer, Nycomed, Roche and Servier. Conflicts of interest: D. Dumitrescu declares honoraria for lectures and/or consultancy from Actelion, AstraZeneca, Bayer, GlaxoSmithKline, Janssen, MSD, Novartis, Pfizer and Servier. Conflicts of interest: I. Tsangaris has received fees from Actelion, Bayer, ELPEN, GlaxoSmithKline, Janssen, MSD, Pfizer and United Therapeutics. Conflicts of interest: A. Vonk-Noordegraaf reports receiving fees for lectures and/or consultations from Actelion, Bayer, GlaxoSmithKline, Janssen, MSD and Pfizer. Conflicts of interest: S. Ulrich reports personal fees from Actelion, Janssen and MSD outside the submitted work. Conflicts of interest: H. Klose has received speaker fees and honoraria for consultations from Actelion, Bayer, GlaxoSmithKline, Janssen, MSD, Novartis, Pfizer and United Therapeutics.
Figures

Comment in
-
To be or not to be… treated with initial combination therapy, that is the (PAH) question.Eur Respir J. 2022 Jun 2;59(6):2200390. doi: 10.1183/13993003.00390-2022. Print 2022 Jun. Eur Respir J. 2022. PMID: 35654453 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical