

Bilateral Structural Network Abnormalities in Epilepsy Associated With Bottom-of-Sulcus Dysplasia
- PMID: 34675097
- PMCID: PMC8762587
- DOI: 10.1212/WNL.0000000000013006
Bilateral Structural Network Abnormalities in Epilepsy Associated With Bottom-of-Sulcus Dysplasia
Abstract
Background and objectives: To identify white matter fiber tracts that exhibit structural abnormality in patients with bottom-of-sulcus dysplasia (BOSD) and investigate their association with seizure activity.
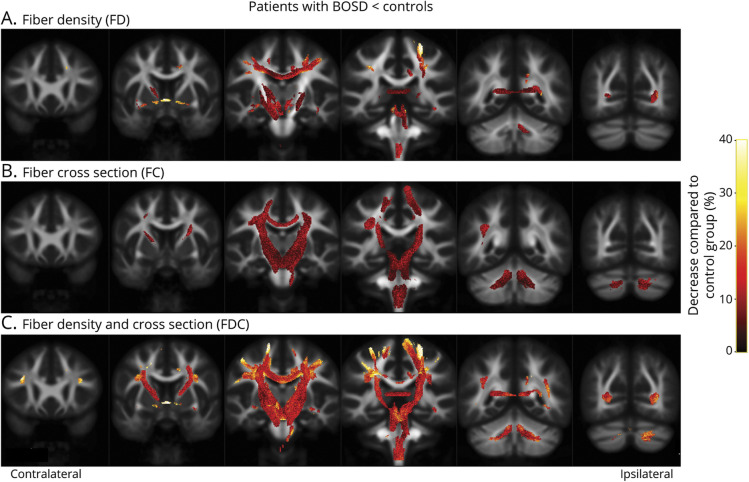
Methods: Whole-brain fixel-based analysis of diffusion MRI data was performed to identify white matter fiber tracts with significant reductions in fiber density and cross-section in patients with BOSD (n = 20) when compared to healthy control participants (n = 40). Results from whole-brain analysis were used to investigate the association of fiber tract abnormality with seizure frequency and epilepsy duration.
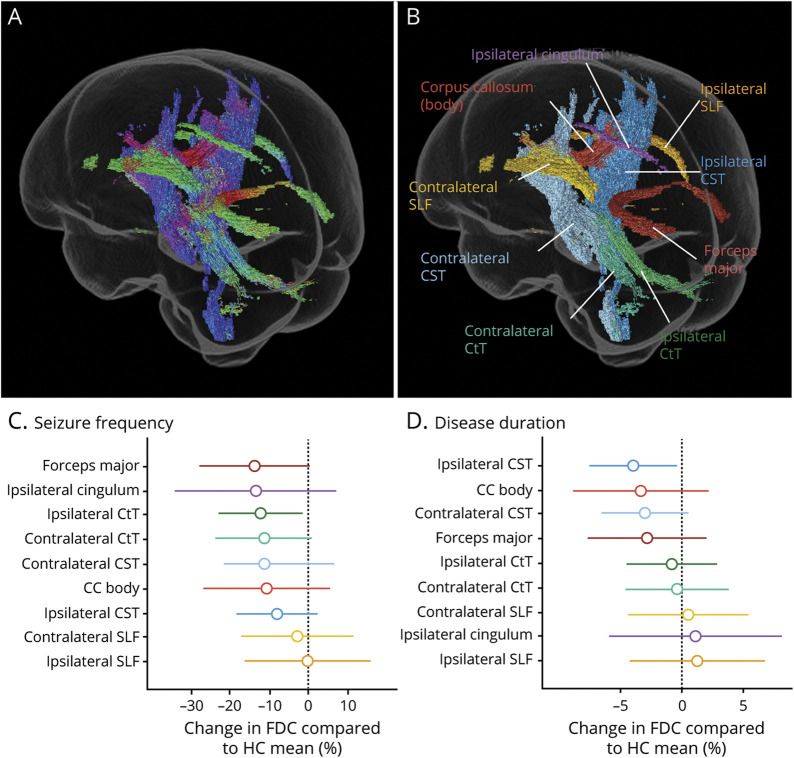
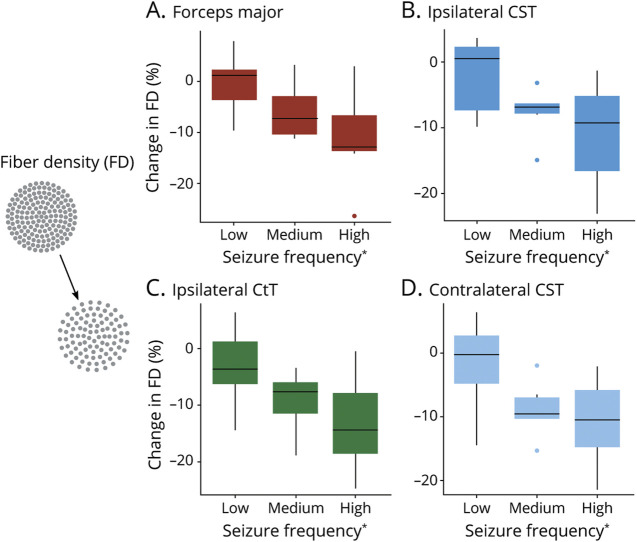
Results: Despite the focal nature of the dysplasia, patients with BOSD showed widespread abnormality in white matter fiber tracts, including the bilateral corticospinal, corticothalamic, and cerebellothalamic tracts, superior longitudinal fasciculi, corpus callosum (body), and the forceps major. This pattern of bilateral connectivity reduction was not related to the laterality of the lesion. Exploratory post hoc analyses showed that high seizure frequency was associated with greater reduction in fiber density at the forceps major, bilateral corticospinal, and cerebellothalamic tracts.
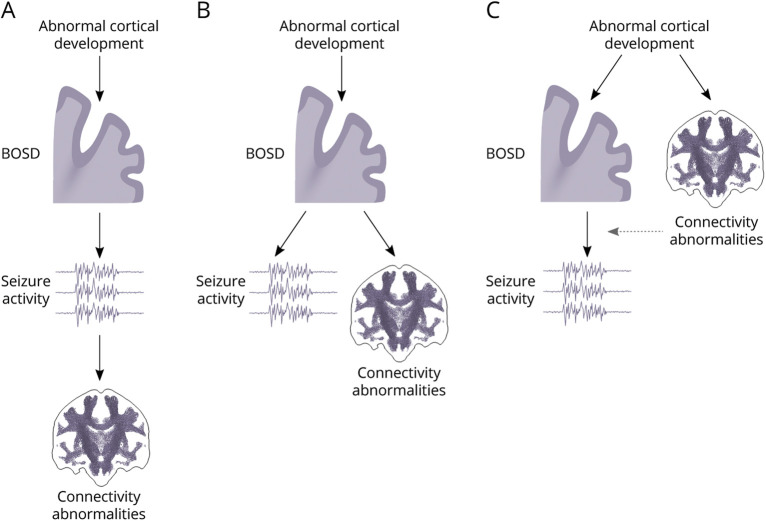
Discussion: We demonstrate evidence of a bilaterally distributed, specific white matter network that is vulnerable to disruption in BOSD. The degree of tract abnormality is partly related to seizure activity, but additional contributors such as the genetic background and effects of treatment or environment have not been excluded.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Bernasconi A. Connectome-based models of the epileptogenic network: a step towards epileptomics? Brain. 2017;140(10):2525-2527. - PubMed
-
- Hong S-J, Bernhardt BC, Gill RS, Bernasconi N, Bernasconi A. The spectrum of structural and functional network alterations in malformations of cortical development. Brain. 2017;140(8):2133-2143. - PubMed
-
- Barkovich AJ, Kuzniecky RI, Jackson GD, Guerrini R, Dobyns WB. A developmental and genetic classification for malformations of cortical development. Neurology. 2005;65(12):1873-1887. - PubMed