

Effect of prewarming on body temperature in short-term bladder or prostatic transurethral resection under general anesthesia: A randomized, double-blind, controlled trial
- PMID: 34675311
- PMCID: PMC8531284
- DOI: 10.1038/s41598-021-00350-2
Effect of prewarming on body temperature in short-term bladder or prostatic transurethral resection under general anesthesia: A randomized, double-blind, controlled trial
Abstract
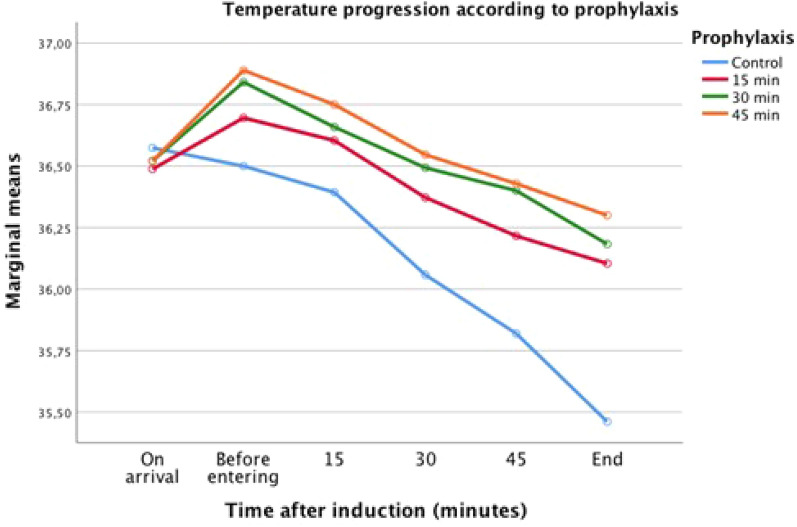
Perioperative hypothermia causes postoperative complications. Prewarming reduces body temperature decrease in long-term surgeries. We aimed to assess the effect of different time-periods of prewarming on perioperative temperature in short-term transurethral resection under general anesthesia. Randomized, double-blind, controlled trial in patients scheduled for bladder or prostatic transurethral resection under general anesthesia. Eligible patients were randomly assigned to receive no-prewarming or prewarming during 15, 30, or 45 min using a forced-air blanket in the pre-anesthesia period. Tympanic temperature was used prior to induction of anesthesia and esophageal temperature intraoperatively. Primary outcome was the difference in core temperature among groups from the induction of general anesthesia until the end of surgery. Repeated measures multivariate analysis of covariance modeled the temperature response at each observation time according to prewarming. We examined modeled contrasts between temperature variables in subjects according to prophylaxis. We enrolled 297 patients and randomly assigned 76 patients to control group, 74 patients to 15-min group, 73 patients to 30-min group, and 74 patients to the 45-min group. Temperature in the control group before induction was 36.5 ± 0.5 °C. After prewarming, core temperature was significantly higher in 15- and 30-min groups (36.8 ± 0.5 °C, p = 0.004; 36.7 ± 0.5 °C, p = 0.041, respectively). Body temperature at the end of surgery was significantly lower in the control group (35.8 ± 0.6 °C) than in the three prewarmed groups (36.3 ± 0.6 °C in 15-min, 36.3 ± 0.5 °C in 30-min, and 36.3 ± 0.6 °C in 45-min group) (p < 0.001). Prewarming prior to short-term transurethral resection under general anesthesia reduced the body temperature drop during the perioperative period. These time-periods of prewarming also reduced the rate of postoperative complications.Study Registration Registered at ClinicalTrials.gov (Identifier: NCT03630887).
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
