

IL-1-driven stromal-neutrophil interactions define a subset of patients with inflammatory bowel disease that does not respond to therapies
- PMID: 34675383
- PMCID: PMC8604730
- DOI: 10.1038/s41591-021-01520-5
IL-1-driven stromal-neutrophil interactions define a subset of patients with inflammatory bowel disease that does not respond to therapies
Abstract
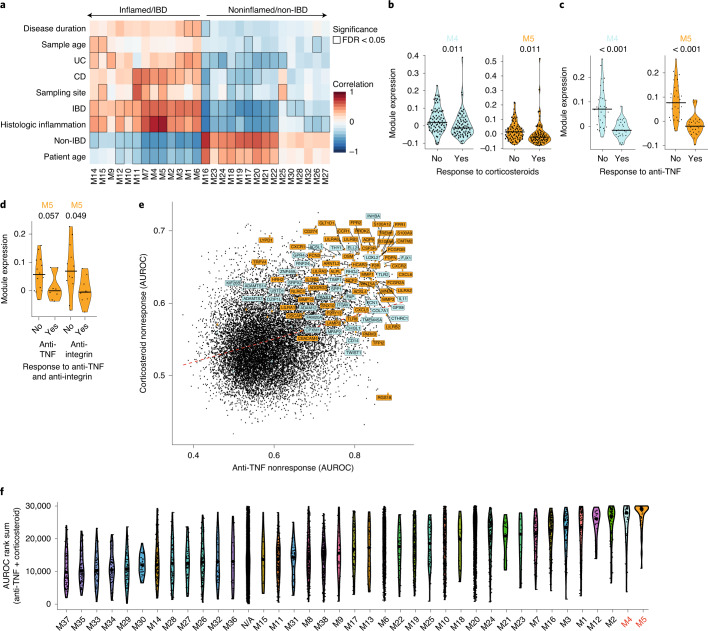
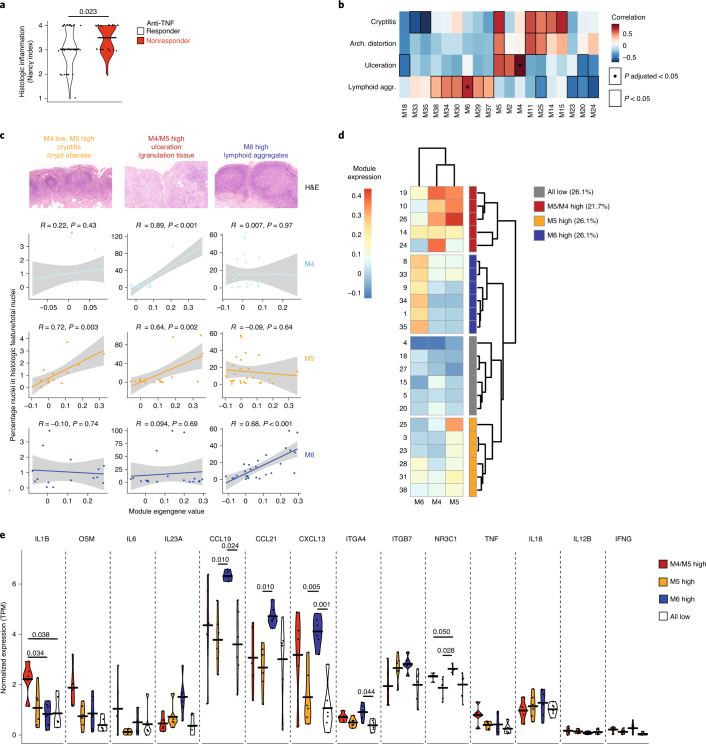
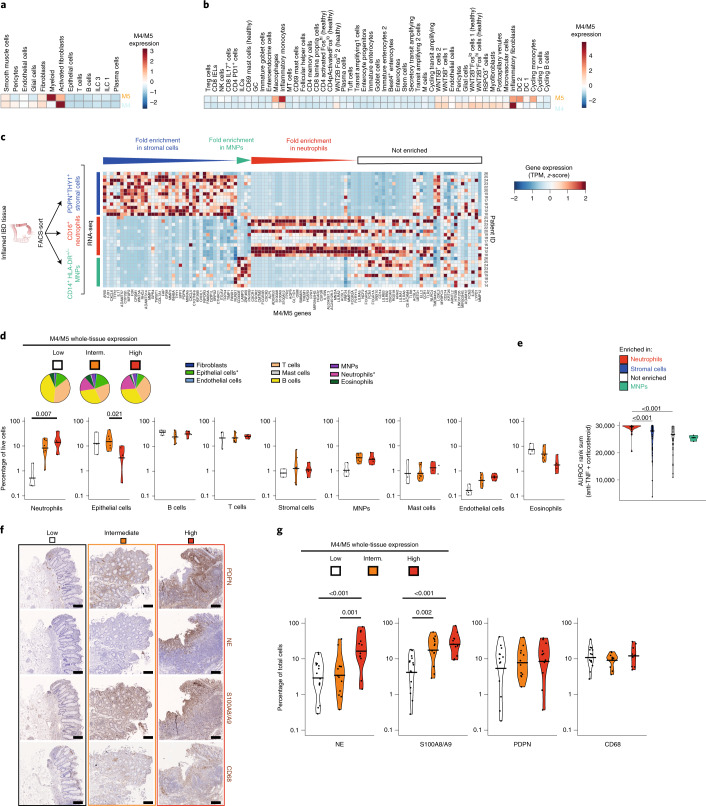
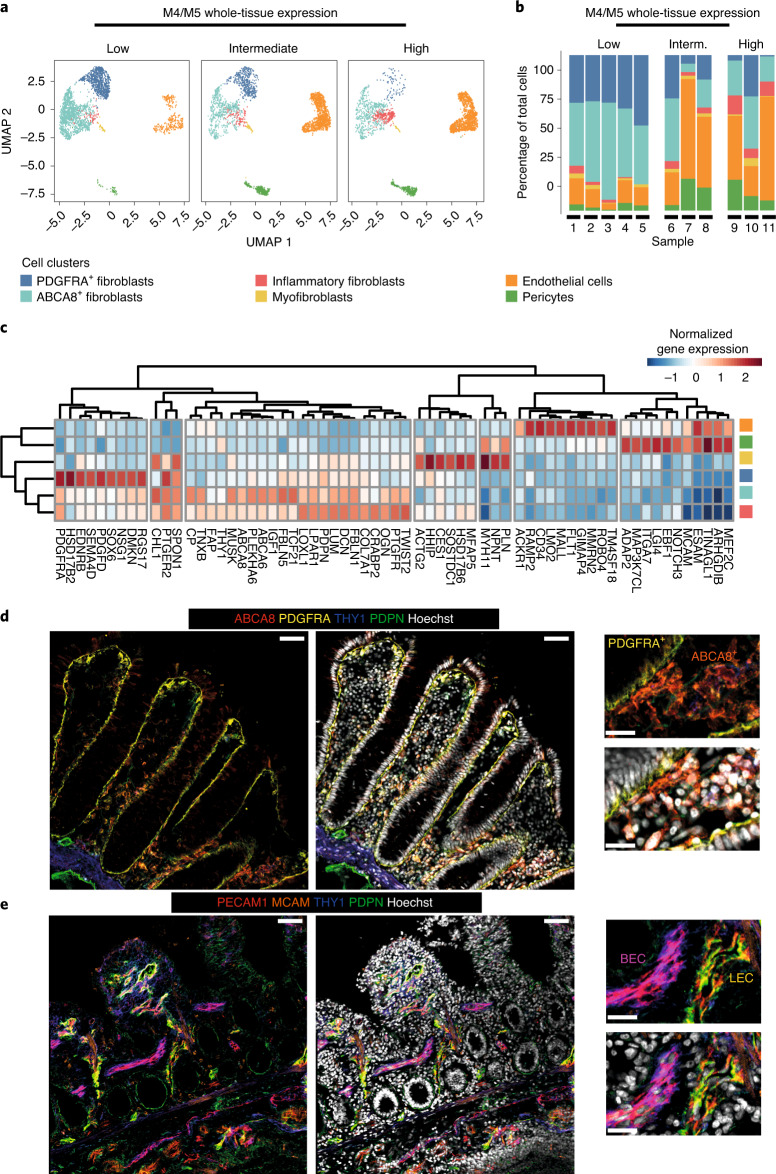
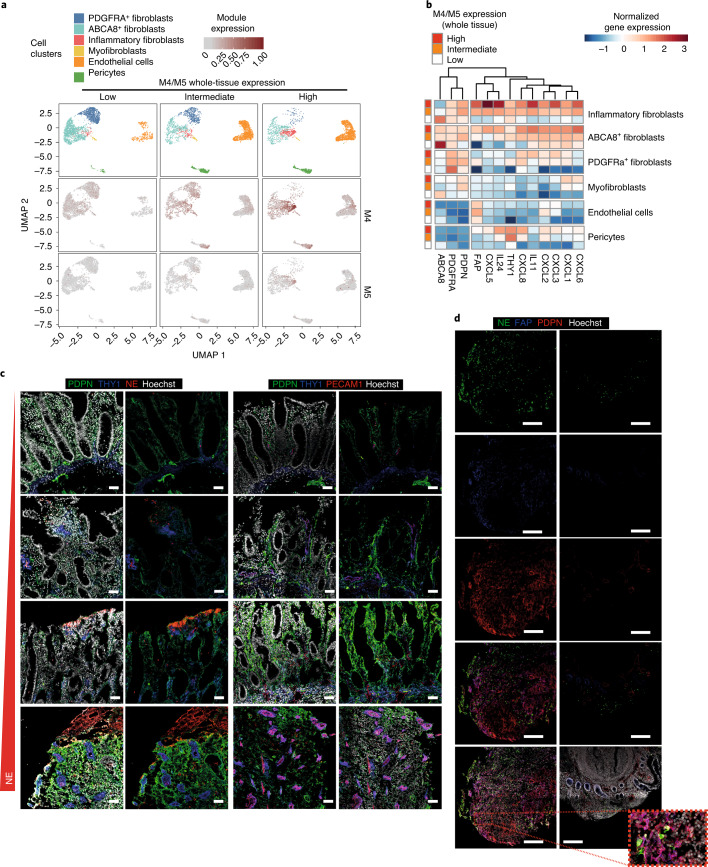
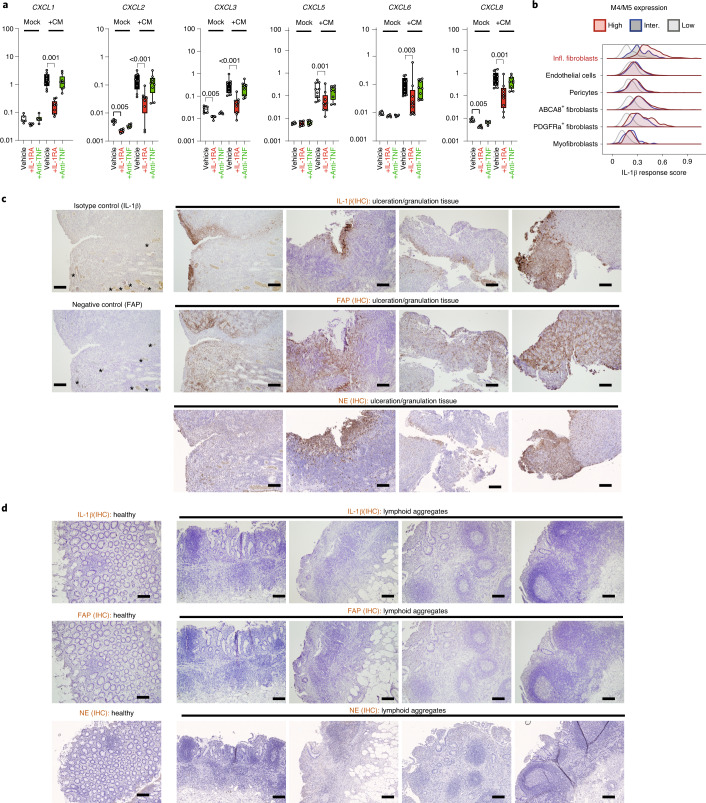
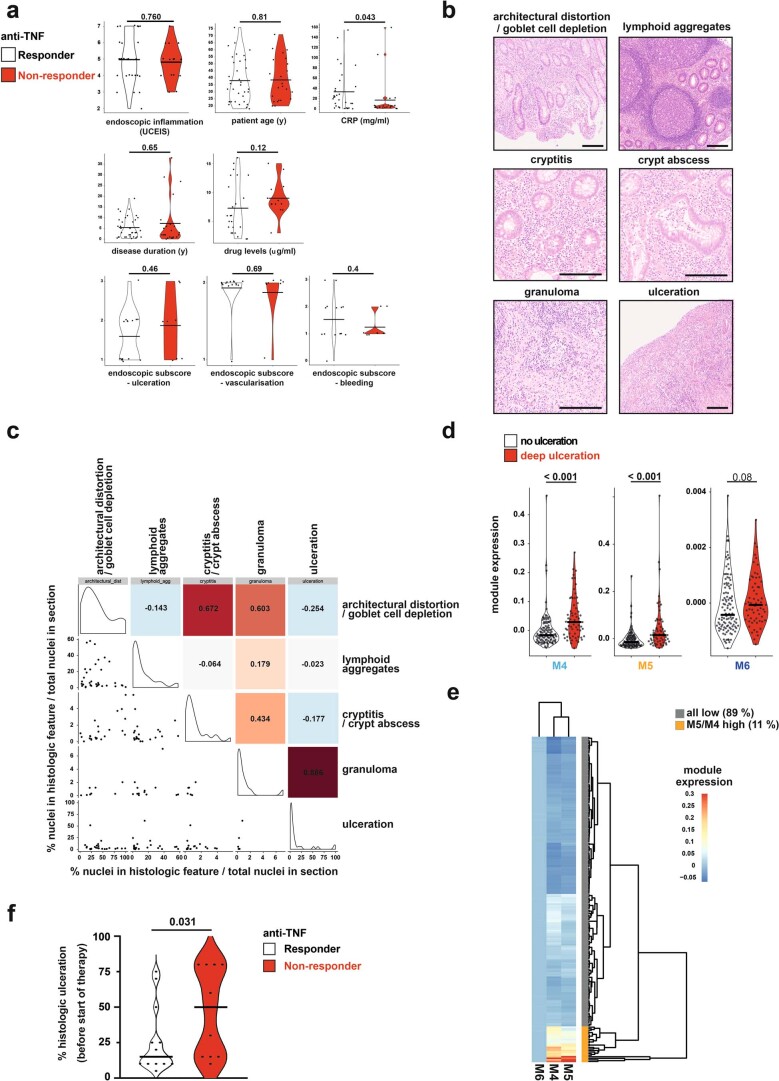
Current inflammatory bowel disease (IBD) therapies are ineffective in a high proportion of patients. Combining bulk and single-cell transcriptomics, quantitative histopathology and in situ localization across three cohorts of patients with IBD (total n = 376), we identify coexpressed gene modules within the heterogeneous tissular inflammatory response in IBD that map to distinct histopathological and cellular features (pathotypes). One of these pathotypes is defined by high neutrophil infiltration, activation of fibroblasts and vascular remodeling at sites of deep ulceration. Activated fibroblasts in the ulcer bed display neutrophil-chemoattractant properties that are IL-1R, but not TNF, dependent. Pathotype-associated neutrophil and fibroblast signatures are increased in nonresponders to several therapies across four independent cohorts (total n = 343). The identification of distinct, localized, tissular pathotypes will aid precision targeting of current therapeutics and provides a biological rationale for IL-1 signaling blockade in ulcerating disease.
© 2021. The Author(s).
Conflict of interest statement
F.M.P. received research support from Roche and Janssen, and consulting fees from GSK, Novartis and Genentech. H.H.U. received research support or consultancy fees from Janssen, Eli Lilly, UCB Pharma, BMS/Celgene, MiroBio, Mestag and OMass. S.P.T. received research support from AbbVie, Buhlmann, Celgene, IOIBD, Janssen, Lilly, Pfizer, Takeda, UCB, Vifor and the Norman Collisson Foundation; consulting fees from AbbVie, Allergan, Αbiomics, Amgen, Arena, Asahi, Astellas, Biocare, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Buhlmann, Celgene, Chemocentryx, Cosmo, Enterome, Ferring, Giuliani SpA, GSK, Genentech, Immunocore, Immunometabolism, Indigo, Janssen, Lexicon, Lilly, Merck, MSD, Neovacs, Novartis, NovoNordisk, NPS Pharmaceuticals, Pfizer, Proximagen, Receptos, Roche, Sensyne, Shire, Sigmoid Pharma, SynDermix, Takeda, Theravance, Tillotts, Topivert, UCB, VHsquared, Vifor and Zeria; and speaker fees from AbbVie, Amgen, Biogen, Ferring, Janssen, Pfizer, Shire, Takeda and UCB (no stocks or share options). M.A.J. is an employee of MiroBio Ltd. K.G.L. and A.P.F. are employees of Roche Ltd. All other authors declare no competing interests.
Figures







Comment in
-
Finding the right target for drug-resistant inflammatory bowel disease.Nat Med. 2021 Nov;27(11):1870-1871. doi: 10.1038/s41591-021-01551-y. Nat Med. 2021. PMID: 34750554 No abstract available.
References
-
- Uhlig HH, Powrie F. Translating immunology into therapeutic concepts for inflammatory bowel disease. Annu. Rev. Immunol. 2018;36:755–781. - PubMed
-
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389:1741–1755. - PubMed
-
- Friedrich M, Pohin M, Powrie F. Cytokine networks in the pathophysiology of inflammatory bowel disease. Immunity. 2019;50:992–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
