

A Review for the Practicing Clinician: Hepatorenal Syndrome, a Form of Acute Kidney Injury, in Patients with Cirrhosis
- PMID: 34675586
- PMCID: PMC8502008
- DOI: 10.2147/CEG.S323778
A Review for the Practicing Clinician: Hepatorenal Syndrome, a Form of Acute Kidney Injury, in Patients with Cirrhosis
Abstract
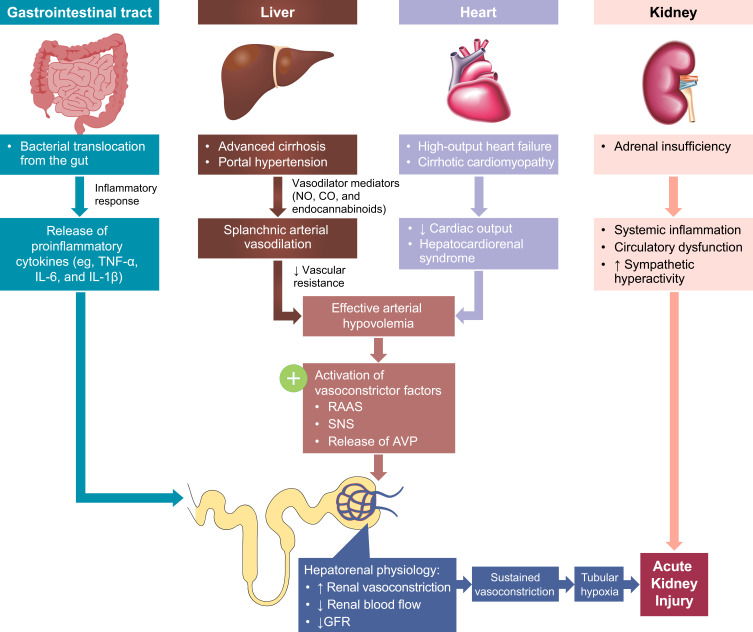
The hepatorenal syndrome type of acute kidney injury (HRS-AKI), formerly known as type 1 hepatorenal syndrome, is a rapidly progressing renal failure that occurs in many patients with advanced cirrhosis and ascites. Accumulating evidence has led to a recent evolution of diagnostic criteria for this serious complication of end-stage liver disease. The aim of this review is to provide an overview of disease-related characteristics and therapeutic management of patients with HRS-AKI. Relevant literature was compiled to support discussion of the pathophysiology, diagnosis, prognosis, associated conditions, prevention, treatment, and management of HRS-AKI. Onset of HRS-AKI is characterized by sudden severe renal vasoconstriction, leading to an acute reduction in glomerular filtration rate and rapid, potentially life-threatening, renal deterioration. Although our understanding of disease pathophysiology continues to evolve, etiology of HRS-AKI likely involves systemic hemodynamic changes caused by liver disease, inflammation, and damage to renal parenchyma. There is currently no gold standard for diagnosis, which typically involves a clinical workup, abdominal imaging, and laboratory assessments. The current consensus definition of HRS-AKI includes proposed diagnostic criteria based on changes in serum creatinine levels tailored for high sensitivity, and rapid detection to accelerate diagnosis and treatment initiation. The only potential cure for HRS-AKI is liver transplantation; however, vasoconstrictive agents and other supportive measures are used as needed to help maintain survival for patients who are awaiting or are ineligible for transplantation. The severity of HRS-AKI, complex pathology, limited treatment options, and range of associated conditions pose significant challenges for both patients and care providers.
Keywords: ascites; cirrhosis; hepatorenal syndrome; liver transplantation; portal hypertension.
© 2021 Chaney.
Conflict of interest statement
The author reports no conflicts of interest in this work.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
