

How Differences in the Disease Process of the COVID-19 Pandemic Pose Challenges to the Delivery of Critical Care Nutrition
- PMID: 34676507
- PMCID: PMC8530202
- DOI: 10.1007/s13668-021-00379-9
How Differences in the Disease Process of the COVID-19 Pandemic Pose Challenges to the Delivery of Critical Care Nutrition
Abstract
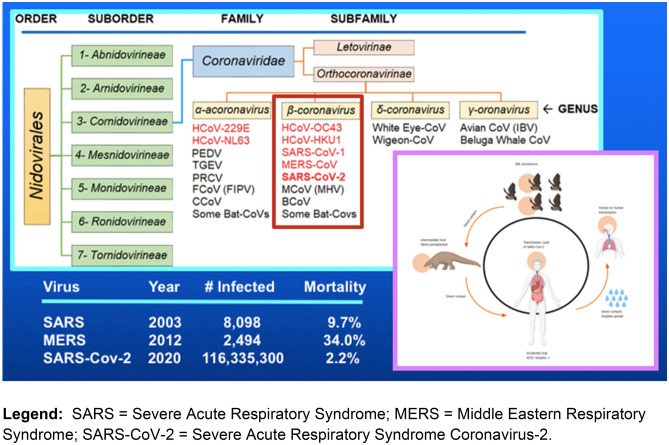
Purpose of review: The COVID-19 pandemic is a unique disease process that has caused unprecedented challenges for intensive care specialists. The hyperinflammatory hypermetabolic nature of the disease and the complexity of its management create barriers to the delivery of nutritional therapy. This review identifies the key differences which characterize this pandemic from other disease processes in critical illness and discusses alternative strategies to enhance success of nutritional support.
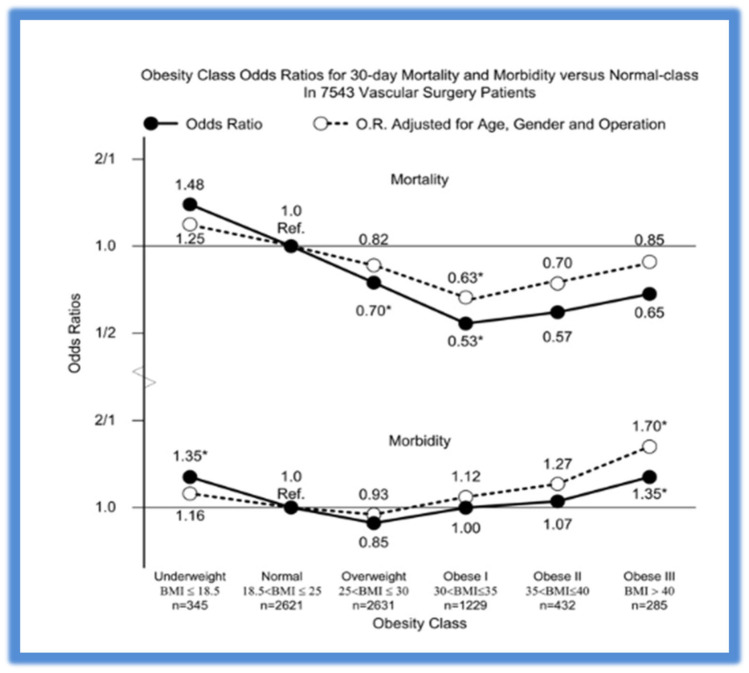
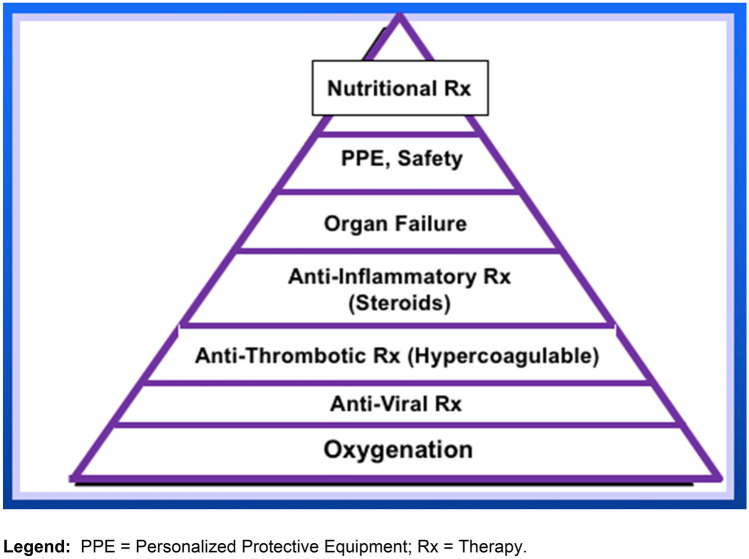
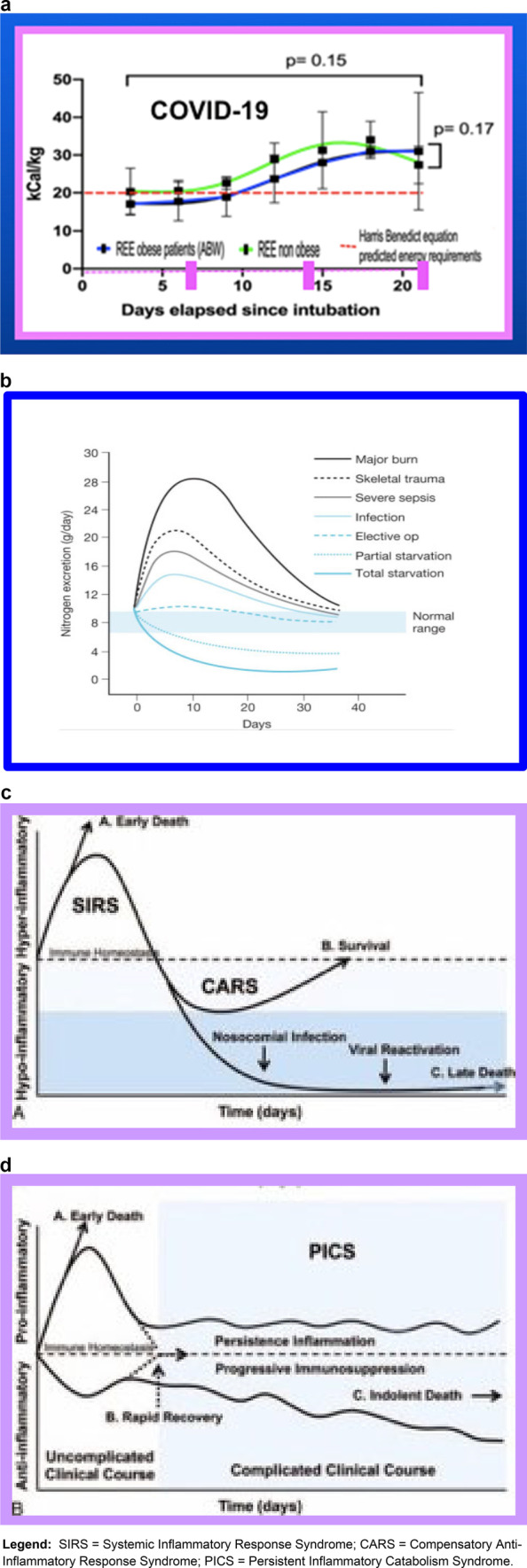
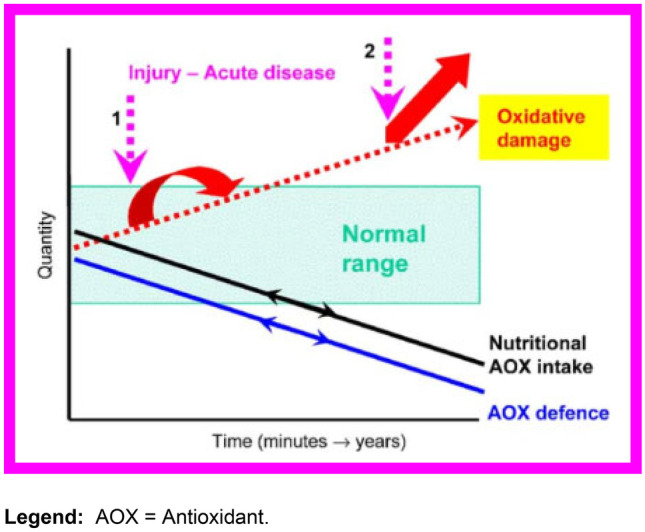
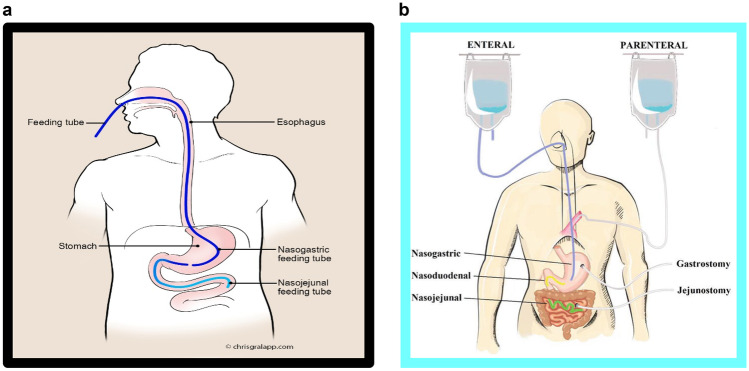
Recent findings: Prolonged hyperinflammation, unlike any previously described pattern of response to injury, causes metabolic perturbations and deterioration of nutritional status. High ventilatory demands, hypercoagulation with the risk of bowel ischemia, and threat of aspiration in patients with little or no pulmonary reserve, thwart initial efforts to provide early enteral nutrition (EN). The obesity paradox is invalidated, tolerance of EN is limited, intensivists are reluctant to add supplemental parenteral nutrition (PN), and efforts to give sufficient nutritional therapy remain a low priority. The nature of the disease and difficulties providing traditional critical care nutrition lead to dramatic deterioration of nutritional status. Institutions should not rely on insufficient gastric feeding alone but focus instead on redoubling efforts to provide postpyloric deep duodenal/jejunal EN or re-examine the role of supplemental PN in this population of patients with such severe critical illness.
Keywords: COVID-19 disease; Coronavirus; Enteral nutrition; Malnutrition; Nutritional therapy; Parenteral nutrition; SARS-CoV-2.
© 2021. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Figures
References
Papers of particular interest, published recently, have been highlighted as:
• Of importance
-
- • Martindale R, Patel JJ, Taylor B, Arabi YM, Warren M, McClave SA. Nutrition therapy in critically ill patients with coronavirus disease 2019. JPEN J Parenter Enteral Nutr. 2020;44(7):1174–1184. This guidance was the first nutritional guidance from ASPEN for critically ill COVID-19 patients. - PMC - PubMed
-
- • McClave SA, Taylor BE, Martindale RG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016;40(2):159–211. (This is the most recent guideline from ASPEN and SCCM on provision and assessment of nutrition in the critically ill patients. The COVID-19 guidance (reference 1) was mainly based on this guidline.) - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous