

Acute and Chronic Effects of COVID-19 on the Cardiovascular System
- PMID: 34677197
- PMCID: PMC8541609
- DOI: 10.3390/jcdd8100128
Acute and Chronic Effects of COVID-19 on the Cardiovascular System
Abstract
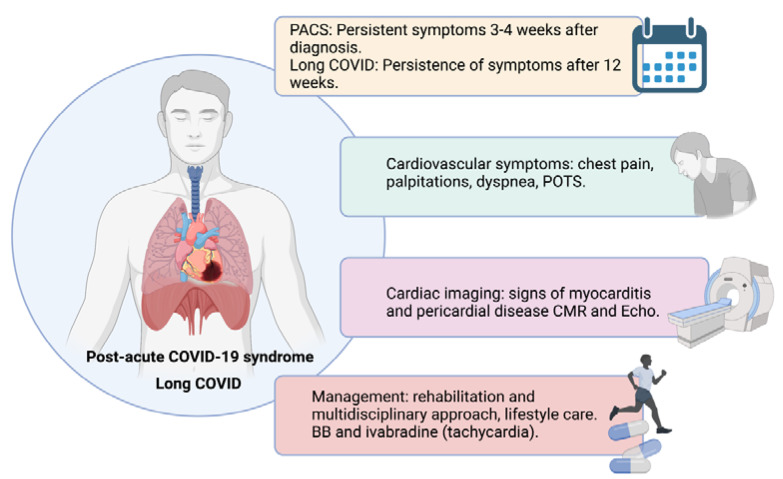
COVID-19 has shown significant morbidity with the involvement of multiple systems, including the cardiovascular system. Cardiovascular manifestations in the acute phase can include myocardial injury itself, myocardial infarction, venous thromboembolic events, myocarditis, Takotsubo syndrome, and different arrhythmic events. Myocardial injury defined by the rise of cardiac biomarkers in blood has been found in multiple studies with a prevalence of about 20%. Its presence is related to worse clinical outcomes and in-hospital mortality. The mechanisms of myocardial injury have been the subject of intense research but still need to be clarified. The characterization of the cardiac affectation with echocardiography and cardiac magnetic resonance has found mixed results in different studies, with a striking incidence of imaging criteria for myocarditis. Regarding post-acute and chronic follow-up results, the persistence of symptoms and imaging changes in recovered COVID-19 patients has raised concerns about the duration and the possible significance of these findings. Even though the knowledge about this disease has increased incredibly in the last year, many aspects are still unclear and warrant further research.
Keywords: SARS-CoV-2; coronavirus disease 2019; long-term outcome; myocardial infarction; myocardial injury; myocarditis; pulmonary embolism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Ortega-Paz L., Capodanno D., Montalescot G., Angiolillo D.J. Coronavirus Disease 2019–Associated Thrombosis and Coagulopathy: Review of the Pathophysiological Characteristics and Implications for Antithrombotic Management. J. Am. Heart Assoc. 2021;10:e019650. doi: 10.1161/JAHA.120.019650. - DOI - PMC - PubMed
-
- Zhou F., Yu T., Du R., Fan G., Liu Y., Liu Z., Xiang J., Wang Y., Song B., Gu X., et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020;395:1054–1062. doi: 10.1016/S0140-6736(20)30566-3. - DOI - PMC - PubMed
-
- Silverio A., Di Maio M., Citro R., Esposito L., Iuliano G., Bellino M., Baldi C., De Luca G., Ciccarelli M., Vecchione C., et al. Cardiovascular risk factors and mortality in hospitalized patients with COVID-19: Systematic review and meta-analysis of 45 studies and 18,300 patients. BMC Cardiovasc. Disord. 2021;21:1–13. doi: 10.1186/s12872-020-01816-3. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
