

Factors Associated With Low-Value Cancer Screenings in the Veterans Health Administration
- PMID: 34677595
- PMCID: PMC8536952
- DOI: 10.1001/jamanetworkopen.2021.30581
Factors Associated With Low-Value Cancer Screenings in the Veterans Health Administration
Abstract
Importance: Most clinical practice guidelines recommend stopping cancer screenings when risks exceed benefits, yet low-value screenings persist. The Veterans Health Administration focuses on improving the value and quality of care, using a patient-centered medical home model that may affect cancer screening behavior.
Objective: To understand rates and factors associated with outpatient low-value cancer screenings.
Design, setting, and participants: This cohort study assessed the receipt of low-value cancer screening and associated factors among 5 993 010 veterans. Four measures of low-value cancer screening defined by validated recommendations of practices to avoid were constructed using administrative data. Patients with cancer screenings in 2017 at Veterans Health Administration primary care clinics were included. Excluded patients had recent symptoms or historic high-risk diagnoses that may affect test appropriateness (eg, melena preceding colonoscopy). Data were analyzed from December 23, 2019, to June 21, 2021.
Exposures: Receipt of cancer screening test.
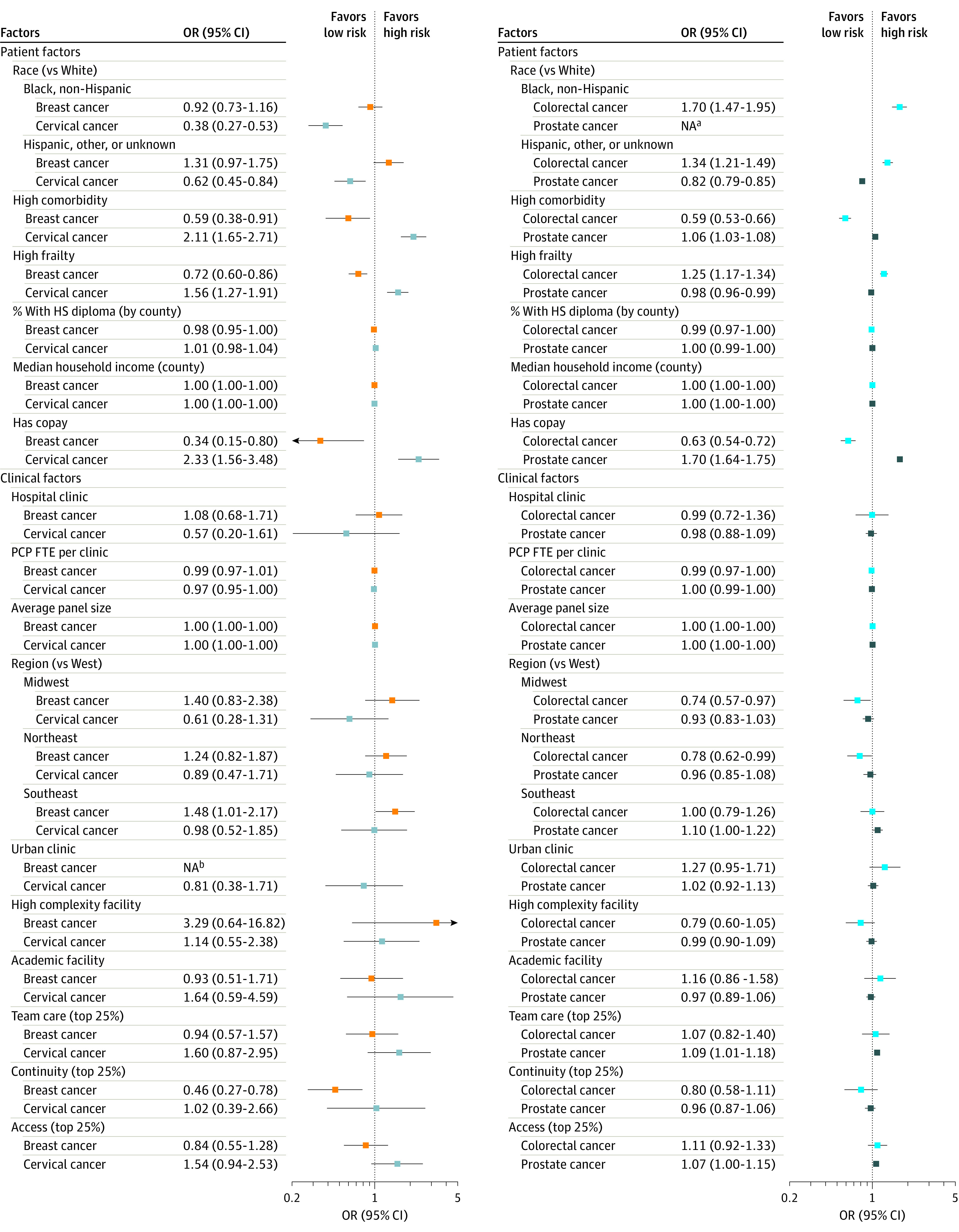
Main outcomes and measures: Low-value screenings were defined as occurring for average-risk patients outside of guideline-recommended ages or if the 1-year mortality risk estimated using a previously validated score was at least 50%. Factors evaluated in multivariable regression models included patient, clinician, and clinic characteristics and patient-centered medical home domain performance for team-based care, access, and continuity previously developed from administrative and survey data.
Results: Of 5 993 010 veterans (mean [SD] age, 63.1 [16.8] years; 5 496 976 men [91.7%]; 1 027 836 non-Hispanic Black [17.2%] and 4 539 341 non-Hispanic White [75.7%] race and ethnicity) enrolled in primary care, 903 612 of 4 647 479 men of average risk (19.4%) underwent prostate cancer screening; 299 765 of 5 770 622 patients of average risk (5.2%) underwent colorectal cancer screening; 21 930 of 469 045 women of average risk (4.7%) underwent breast cancer screening; and 65 511 of 458 086 women of average risk (14.3%) underwent cervical cancer screening. Of patients screened, low-value testing was rare for 3 cancers, with receipt of a low-value test in 633 of 21 930 of women screened for breast cancer (2.9%), 630 of 65 511 of women screened for cervical cancer (1.0%), and 6790 of 299 765 of patients screened for colorectal cancer (2.3%). However, 350 705 of 4 647 479 of screened men (7.5%) received a low-value prostate cancer test. Patient race and ethnicity, sociodemographic factors, and illness burden were significantly associated with likelihood of receipt of low-value tests among screened patients. No single patient-, clinician-, or clinic-level factor explained the receipt of a low-value test across cancer screening cohorts.
Conclusions and relevance: This large cohort study found that low-value breast, cervical, and colorectal cancer screenings were rare in the Veterans Health Administration, but more than one-third of patients screened for prostate cancer were tested outside of clinical practice guidelines. Guideline-discordant care has quality implications and is not consistently explained by associated multilevel factors.
Conflict of interest statement
Figures
Similar articles
-
Assessment of Care Cascades Following Low-Value Prostate-Specific Antigen Testing Among Veterans Dually Enrolled in the US Veterans Health Administration and Medicare Systems.JAMA Netw Open. 2022 Dec 1;5(12):e2247180. doi: 10.1001/jamanetworkopen.2022.47180. JAMA Netw Open. 2022. PMID: 36520431 Free PMC article.
-
Association Between Guideline-Discordant Prostate Cancer Imaging Rates and Health Care Service Among Veterans and Medicare Recipients.JAMA Netw Open. 2018 Aug 3;1(4):e181172. doi: 10.1001/jamanetworkopen.2018.1172. JAMA Netw Open. 2018. PMID: 30646111 Free PMC article.
-
Impact of age and comorbidity on colorectal cancer screening among older veterans.Ann Intern Med. 2009 Apr 7;150(7):465-73. doi: 10.7326/0003-4819-150-7-200904070-00006. Ann Intern Med. 2009. PMID: 19349631 Free PMC article.
-
Cancer Screening Recommendations During the COVID-19 Pandemic: Scoping Review.JMIR Cancer. 2022 Feb 24;8(1):e34392. doi: 10.2196/34392. JMIR Cancer. 2022. PMID: 35142621 Free PMC article.
-
Age-Appropriate Cancer Screenings Through a Dermatology Len.WMJ. 2023 Sep;122(4):262-267. WMJ. 2023. PMID: 37768766 Review.
Cited by
-
Structural Racism in Cervical Cancer Care and Survival Outcomes: A Systematic Review of Inequities and Barriers.Curr Epidemiol Rep. 2025;12(1):7. doi: 10.1007/s40471-025-00360-y. Epub 2025 Apr 26. Curr Epidemiol Rep. 2025. PMID: 40297709 Free PMC article. Review.
-
Cancer screening outside of age recommendations: a population-based study.BMC Public Health. 2025 May 6;25(1):1660. doi: 10.1186/s12889-025-22848-4. BMC Public Health. 2025. PMID: 40329270 Free PMC article.
-
Lung Cancer Screening Among U.S. Military Veterans by Health Status and Race and Ethnicity, 2017-2020: A Cross-Sectional Population-Based Study.AJPM Focus. 2023 Feb 9;2(2):100084. doi: 10.1016/j.focus.2023.100084. eCollection 2023 Jun. AJPM Focus. 2023. PMID: 37790642 Free PMC article.
-
Racial Disparities in Low-Value Care in the Last Year of Life for Medicare Beneficiaries With Neurodegenerative Disease.Neurol Clin Pract. 2024 Apr;14(2):e200273. doi: 10.1212/CPJ.0000000000200273. Epub 2024 Mar 15. Neurol Clin Pract. 2024. PMID: 38524836 Free PMC article.
-
Racial differences in low value care among older adult Medicare patients in US health systems: retrospective cohort study.BMJ. 2023 Oct 25;383:e074908. doi: 10.1136/bmj-2023-074908. BMJ. 2023. PMID: 37879735 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
