

Quality of Life as a Mediator between Cancer Stage and Long-Term Mortality in Nasopharyngeal Cancer Patients Treated with Intensity-Modulated Radiotherapy
- PMID: 34680211
- PMCID: PMC8533735
- DOI: 10.3390/cancers13205063
Quality of Life as a Mediator between Cancer Stage and Long-Term Mortality in Nasopharyngeal Cancer Patients Treated with Intensity-Modulated Radiotherapy
Abstract
Background: Quality of life (QoL) attained before, during, or after treatments is recognized as a vital factor associated with therapeutic benefits in cancer patients. This nasopharyngeal cancer (NPC) patient longitudinal study assessed the relationship among QoL, cancer stage, and long-term mortality in patients with nasopharyngeal carcinoma (NPC) treated with intensity-modulated radiotherapy (IMRT).
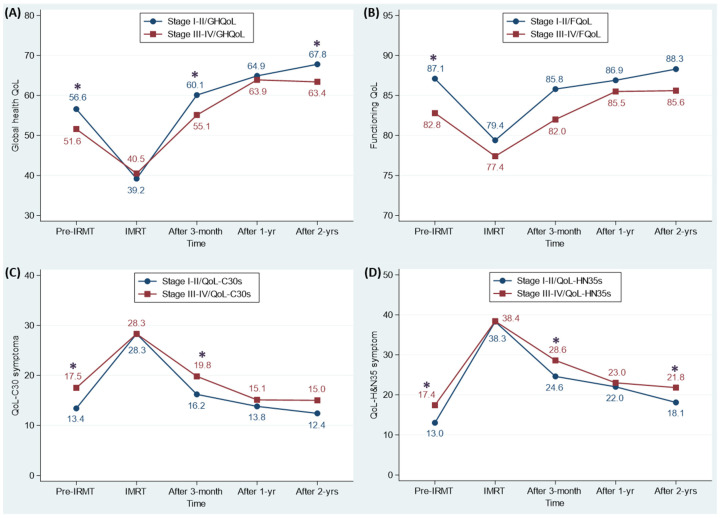
Patients and methods: The European Organization for Research and Treatment of Cancer (EORTC) core QoL questionnaire (QLQ-C30) and the head and neck cancer-specific QoL questionnaire module (QLQ-HN35) were employed to evaluate four-dimensional QoL outcomes at five time points: pre- (n = 682), during (around 40 Gy) (n = 675), 3 months (n = 640), 1 year (n = 578) and 2 years post-IMRT (n = 505), respectively, for 682 newly diagnosed NPC patients treated between 2003 and 2017 at a single institute. The median followed-up time was 7.5 years, ranging from 0.3 to 16.1 years. Generalized estimating equations, multivariable proportional hazards models, and Baron and Kenny's method were used to assess the investigated effects.
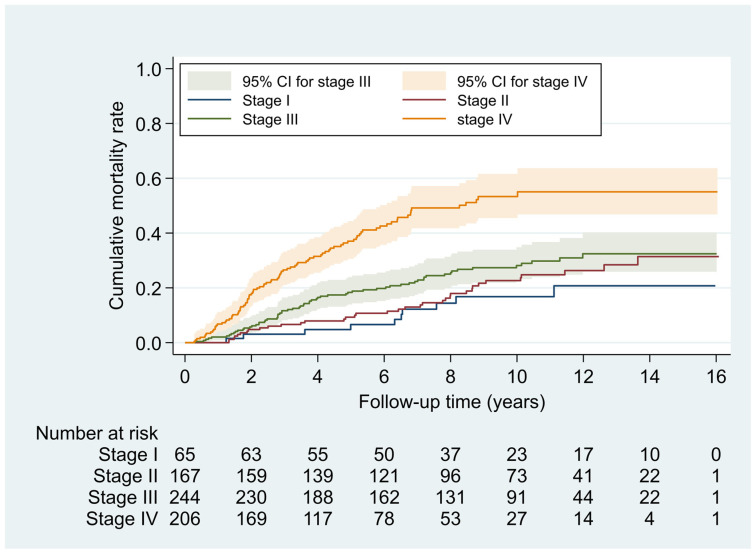
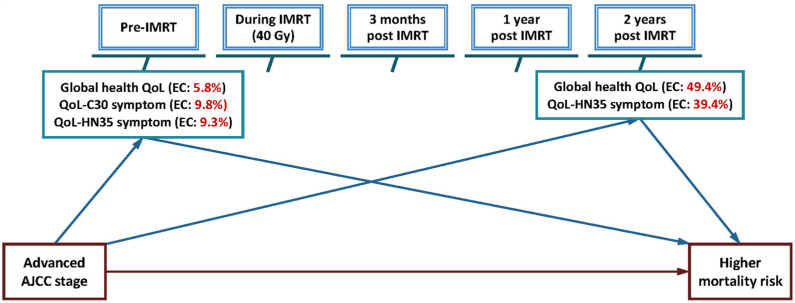
Results: Advanced AJCC stage (III-IV) patients revealed a 2.26-fold (95% CI-1.56 to 3.27) higher covariate-adjusted mortality risk than early-stage (I-II) patients. Compared with during IMRT, advanced-stage patients had a significantly low global health QoL and a significantly high QoL-HN35 symptom by a large magnitude at pre-, 3 months, and 2 years post-IMRT. QoL scales at pre-IMRT, 1 year, and 2 years post-IMRT were significantly associated with mortality. The effect changes of mortality risk explained by global health QoL, QoL-C30, and QoL-HN35 symptom were 5.8-9.8% at pre-IMRT but at 2 years post-IMRT were 39.4-49.4% by global health QoL and QoL-HN35 symptoms.
Conclusions: We concluded advanced cancer stage correlates with a long-term high mortality in NPC patients treated with IMRT and the association is partially intermediated by QoL at pre-IMRT and 2 years post-IMRT. Therefore, QoL-HN35 symptom and global health QoL-dependent medical support and care should be focused and tailored at 2 years post-IMRT.
Keywords: Baron and Kenny’s method; intensity modulated radiotherapy; mediator; mortality; nasopharyngeal carcinoma; quality of life.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kanno M., Narita N., Fujimoto Y., Wakisaka N., Yoshizaki T., Kodaira T., Makita C., Sato Y., Yamazaki K., Wakaoka T., et al. Third Epidemiological Analysis of Nasopharyngeal Carcinoma in the Central Region of Japan from 2006 to 2015. Cancers. 2019;11:1180. doi: 10.3390/cancers11081180. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
