

Combining Hypermethylated RASSF1A Detection Using ddPCR with miR-371a-3p Testing: An Improved Panel of Liquid Biopsy Biomarkers for Testicular Germ Cell Tumor Patients
- PMID: 34680375
- PMCID: PMC8534014
- DOI: 10.3390/cancers13205228
Combining Hypermethylated RASSF1A Detection Using ddPCR with miR-371a-3p Testing: An Improved Panel of Liquid Biopsy Biomarkers for Testicular Germ Cell Tumor Patients
Abstract
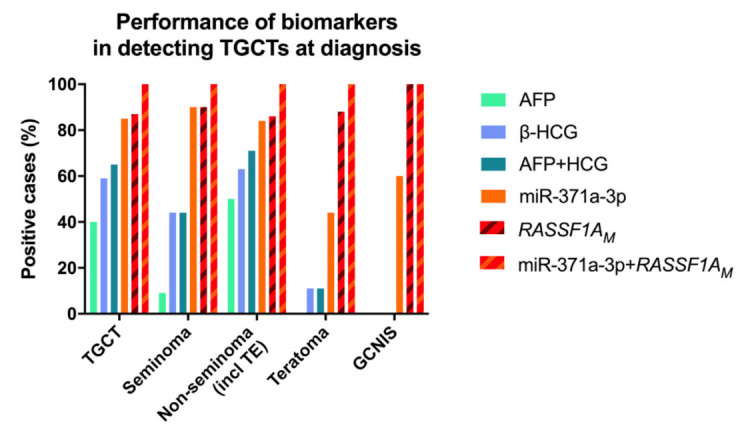
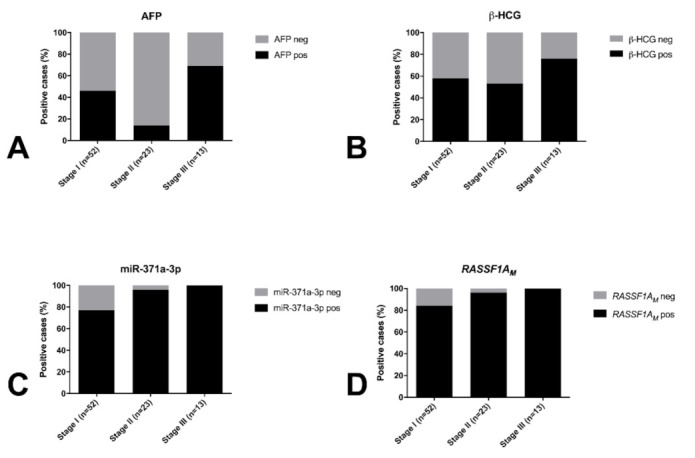
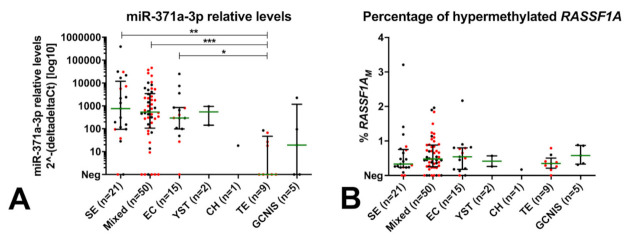
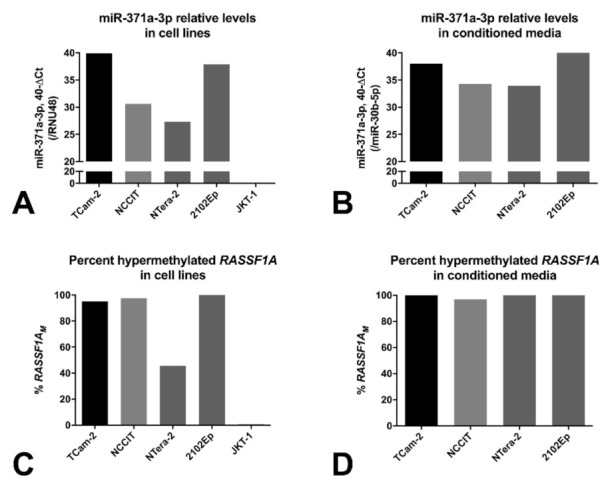
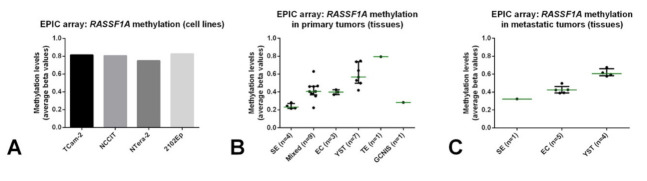
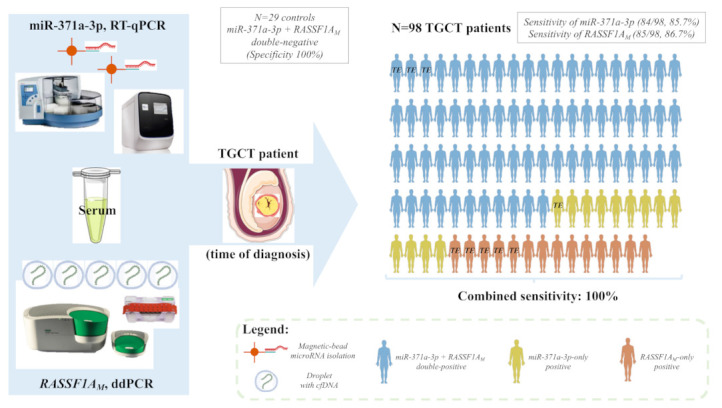
The classical serum tumor markers used routinely in the management of testicular germ cell tumor (TGCT) patients-alpha fetoprotein (AFP) and human chorionic gonadotropin (HCG)-show important limitations. miR-371a-3p is the most recent promising biomarker for TGCTs, but it is not sufficiently informative for detection of teratoma, which is therapeutically relevant. We aimed to test the feasibility of hypermethylated RASSF1A (RASSF1AM) detected in circulating cell-free DNA as a non-invasive diagnostic marker of testicular germ cell tumors, combined with miR-371a-3p. A total of 109 serum samples of patients and 29 sera of healthy young adult males were included, along with representative cell lines and tumor tissue samples. We describe a novel droplet digital polymerase chain reaction (ddPCR) method for quantitatively assessing RASSF1AM in liquid biopsies. Both miR-371a-3p (sensitivity = 85.7%) and RASSF1AM (sensitivity = 86.7%) outperformed the combination of AFP and HCG (sensitivity = 65.5%) for TGCT diagnosis. RASSF1AM detected 88% of teratomas. In this representative cohort, 14 cases were negative for miR-371a-3p, all of which were detected by RASSF1AM, resulting in a combined sensitivity of 100%. We have described a highly sensitive and specific panel of biomarkers for TGCT patients, to be validated in the context of patient follow-up and detection of minimal residual disease.
Keywords: RASSF1A; biomarkers; droplet digital PCR; germ cell tumors; methylation; miR-371a-3p; microRNAs.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
