

Mastocytosis and Mast Cell Activation Disorders: Clearing the Air
- PMID: 34681933
- PMCID: PMC8540348
- DOI: 10.3390/ijms222011270
Mastocytosis and Mast Cell Activation Disorders: Clearing the Air
Abstract
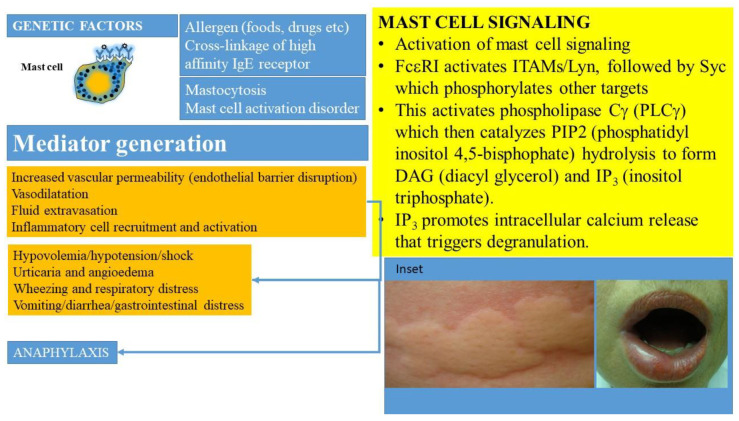
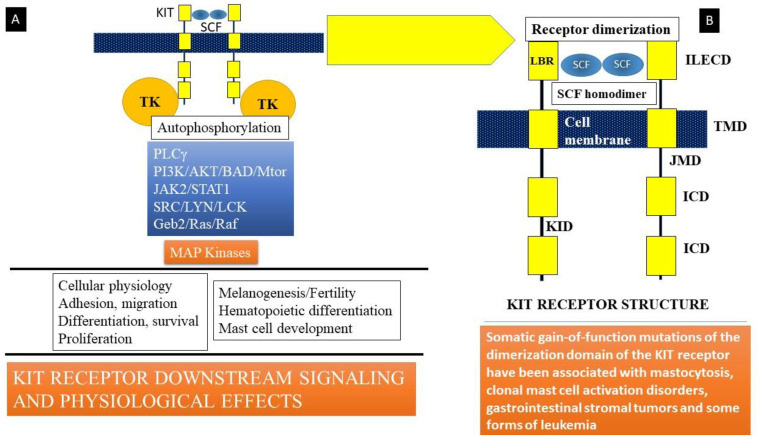
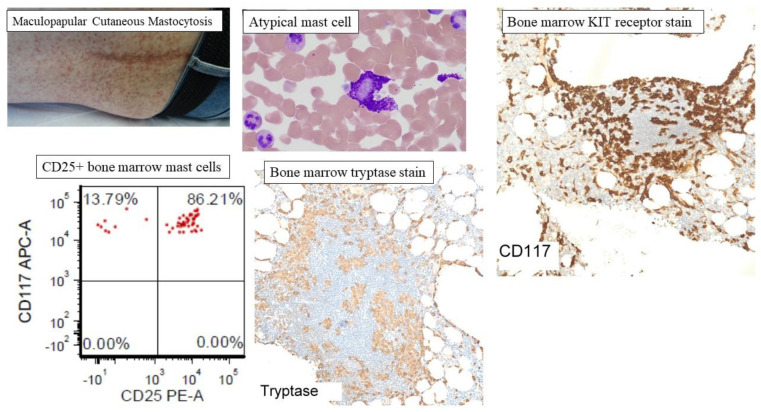
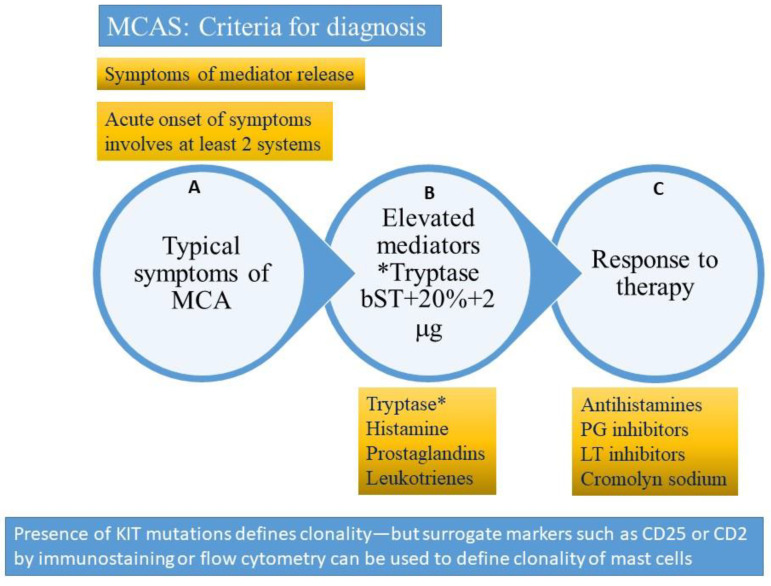
Mast cells are derived from hematopoietic stem cell precursors and are essential to the genesis and manifestations of the allergic response. Activation of these cells by allergens leads to degranulation and elaboration of inflammatory mediators, responsible for regulating the acute dramatic inflammatory response seen. Mast cells have also been incriminated in such diverse disorders as malignancy, arthritis, coronary artery disease, and osteoporosis. There has been a recent explosion in our understanding of the mast cell and the associated clinical conditions that affect this cell type. Some mast cell disorders are associated with specific genetic mutations (such as the D816V gain-of-function mutation) with resultant clonal disease. Such disorders include cutaneous mastocytosis, systemic mastocytosis (SM), its variants (indolent/ISM, smoldering/SSM, aggressive systemic mastocytosis/ASM) and clonal (or monoclonal) mast cell activation disorders or syndromes (CMCAS/MMAS). Besides clonal mast cell activations disorders/CMCAS (also referred to as monoclonal mast cell activation syndromes/MMAS), mast cell activation can also occur secondary to allergic, inflammatory, or paraneoplastic disease. Some disorders are idiopathic as their molecular pathogenesis and evolution are unclear. A genetic disorder, referred to as hereditary alpha-tryptasemia (HαT) has also been described recently. This condition has been shown to be associated with increased severity of allergic and anaphylactic reactions and may interact variably with primary and secondary mast cell disease, resulting in complex combined disorders. The role of this review is to clarify the classification of mast cell disorders, point to molecular aspects of mast cell signaling, elucidate underlying genetic defects, and provide approaches to targeted therapies that may benefit such patients.
Keywords: allergic reaction; anaphylactic shock; angioedema; histamine; hypotension; mast cell; mastocytosis; tryptase.
Conflict of interest statement
None of the authors report a conflict of interest relevant to the publication of this manuscript.
Figures
References
-
- Ghably J., Saleh H., Vyas H., Peiris E., Misra N., Krishnaswamy G. Paul Ehrlich’s mastzellen: A historical perspective of relevant developments in mast cell biology. Methods Mol. Biol. 2015;1220:3–10. - PubMed
-
- Krishnaswamy G., Ajitawi O., Chi D.S. The human mast cell: An overview. Methods Mol. Biol. 2006;315:13–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
