

Recurrence of Hepatic Encephalopathy after TIPS: Effective Prophylaxis with Combination of Lactulose and Rifaximin
- PMID: 34682886
- PMCID: PMC8537523
- DOI: 10.3390/jcm10204763
Recurrence of Hepatic Encephalopathy after TIPS: Effective Prophylaxis with Combination of Lactulose and Rifaximin
Abstract
Background: Transjugular intrahepatic portosystemic shunt (TIPS) implantation is an established procedure to treat portal hypertension with hepatic encephalopathy (HE) as a common complication. There is lack of evidence concerning HE prophylaxis after TIPS.
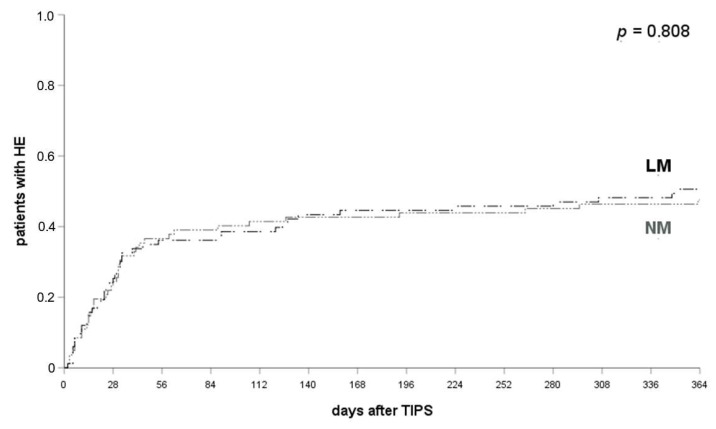
Methods: N = 233 patients receiving TIPS between 2011 and 2018 at a German tertiary care center were included. Of them, 21% (n = 49) had a history of HE. The follow-up period was 12 months. The risk factors of post-TIPS HE were analyzed via multivariate analysis. The efficacy of prophylactic medication regimens was studied. The results show that 35.6% (n = 83) received no medication (NM), 36.5% (n = 85) received lactulose monoprophylaxis (LM), 2.6% (n = 6) rifaximin monoprophylaxis (RM) and 25.3% (n = 59) lactulose and rifaximin (LR) of which 64.4% received l-ornithin-l-aspartate (LOLA) additionally (LR + LOLA) and 36.6% did not (LRonly).
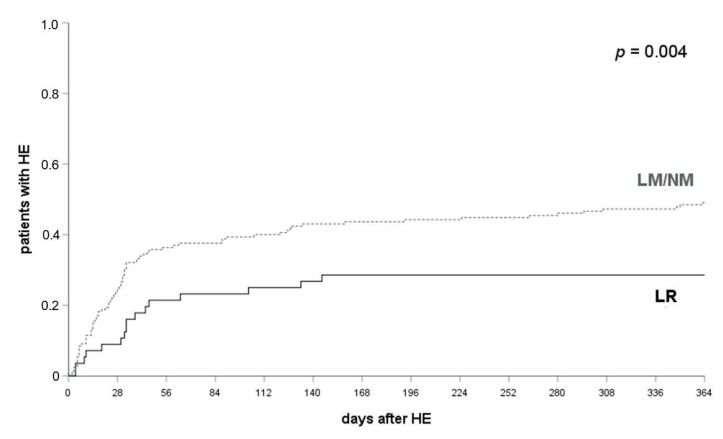
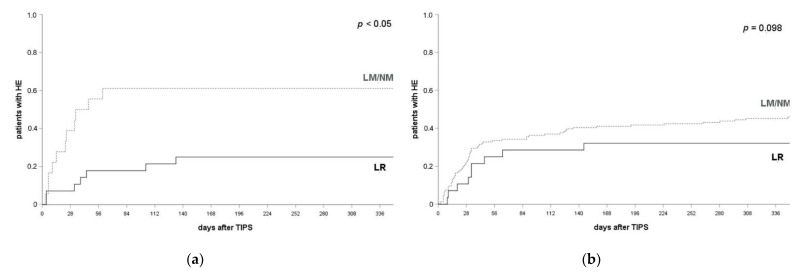
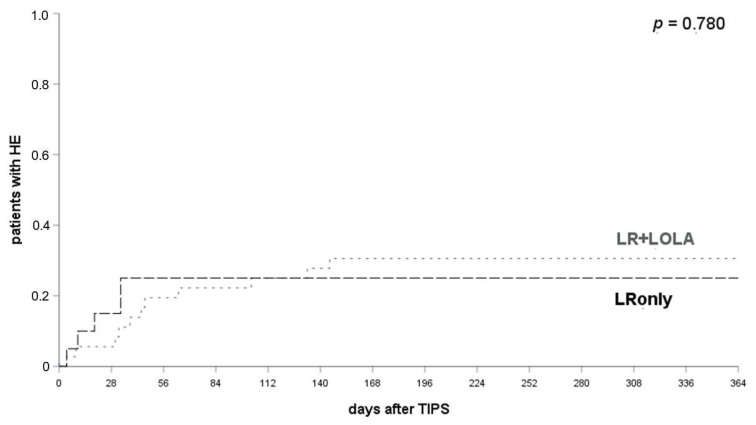
Results: Multivariate analysis revealed higher age (p = 0.003) and HE episodes prior to TIPS (p = 0.004) as risk factors for HE after TIPS. LM has no prophylactic effect. LR prevents HE recurrence at 1, 3 and 12 months after TIPS (p = 0.003, p = 0.003, p = 0.006) but does not prevent HE in patients with no history of HE (p = 0.234, p = 0.483, p = 0.121). LR prevents HE recurrence compared with LM/NM (25.0% vs. 64.7%, p = 0.007) within 12 months after TIPS, whereas de novo occurrence is unaffected (p = 0.098). The additional administration of LOLA to LR has no benefit (LRonly: 25.0%, LR + LOLA: 29.7%, p = 0.780).
Conclusions: Higher age and previous HE are risk factors post-TIPS HE. In patients with HE prior to TIPS, effective prophylaxis of HE is feasible via combination of lactulose and rifaximin with no additional benefit from LOLA.
Keywords: complications of liver cirrhosis; decompensated liver cirrhosis; hepatic encephalopathy; portal hypertension; transjugular intrahepatic portosystemic shunt.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
