

Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients-Insights from the PRoVENT-COVID Observational Study
- PMID: 34682907
- PMCID: PMC8541588
- DOI: 10.3390/jcm10204783
Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients-Insights from the PRoVENT-COVID Observational Study
Abstract
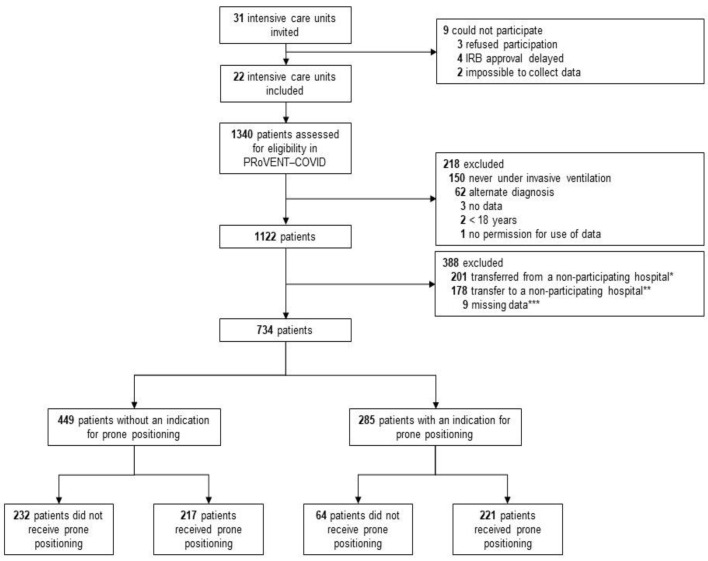
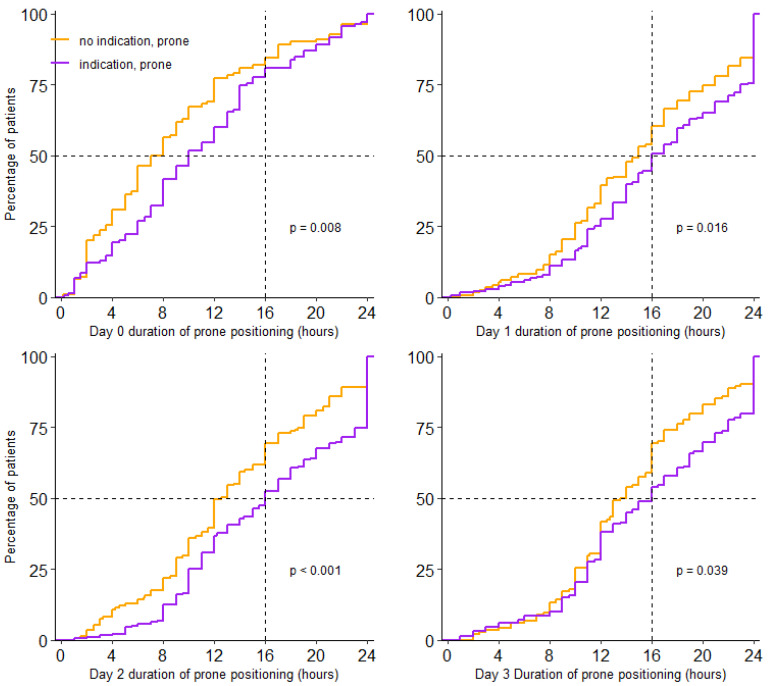
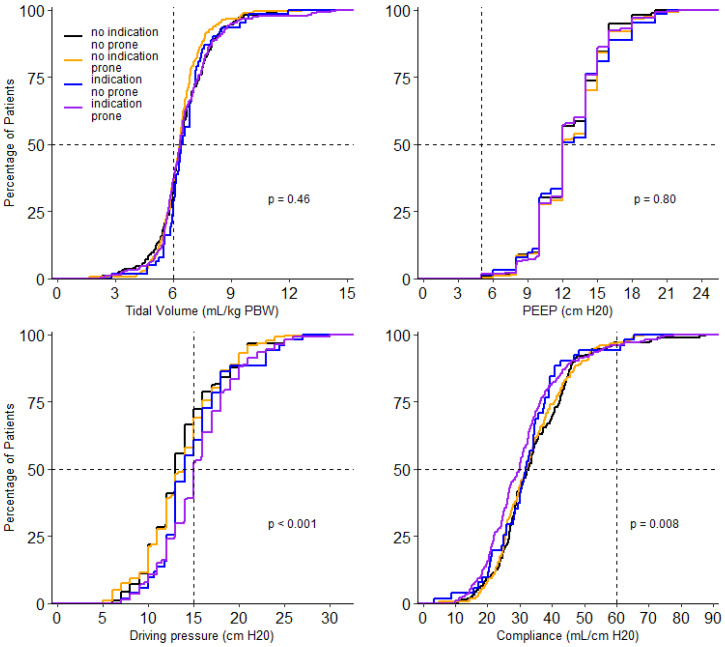
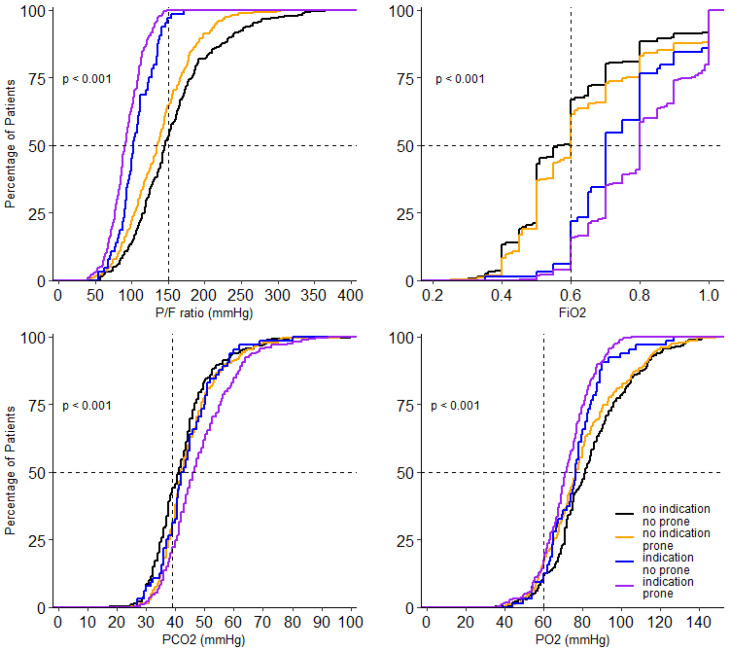
We describe the incidence and practice of prone positioning and determined the association of use of prone positioning with outcomes in invasively ventilated patients with acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19) in a national, multicenter observational study, performed at 22 intensive care units in the Netherlands. Patients were categorized into 4 groups, based on indication for and actual use of prone positioning. The primary outcome was 28-day mortality. Secondary endpoints were 90-day mortality, and ICU and hospital length of stay. In 734 patients, prone positioning was indicated in 60%-the incidence of prone positioning was higher in patients with an indication than in patients without an indication for prone positioning (77 vs. 48%, p = 0.001). Patients were left in the prone position for median 15.0 (10.5-21.0) hours per full calendar day-the duration was longer in patients with an indication than in patients without an indication for prone positioning (16.0 (11.0-23.0) vs. 14.0 (10.0-19.0) hours, p < 0.001). Ventilator settings and ventilation parameters were not different between the four groups, except for FiO2 which was higher in patients having an indication for and actually receiving prone positioning. Our data showed no difference in mortality at day 28 between the 4 groups (HR no indication, no prone vs. no indication, prone vs. indication, no prone vs. indication, prone: 1.05 (0.76-1.45) vs. 0.88 (0.62-1.26) vs. 1.15 (0.80-1.54) vs. 0.96 (0.73-1.26) (p = 0.08)). Factors associated with the use of prone positioning were ARDS severity and FiO2. The findings of this study are that prone positioning is often used in COVID-19 patients, even in patients that have no indication for this intervention. Sessions of prone positioning lasted long. Use of prone positioning may affect outcomes.
Keywords: ARDS; COVID-19; artificial ventilation; coronavirus disease 2019; critical care; intensive care; mortality; prone positioning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Sud S., Friedrich J., Adhikari N.K.J., Taccone P., Mancebo J., Polli F., Latini R., Pesenti A., Curley M., Fernandez R., et al. Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: A systematic review and meta-analysis. Can. Med. Assoc. J. 2014;186:E381–E390. doi: 10.1503/cmaj.140081. - DOI - PMC - PubMed
-
- Constantin J.-M., Jabaudon M., Lefrant J.-Y., Jaber S., Quenot J.-P., Langeron O., Ferrandière M., Grelon F., Seguin P., Ichai C., et al. Personalised mechanical ventilation tailored to lung morphology versus low positive end-expiratory pressure for patients with acute respiratory distress syndrome in France (the LIVE study): A multicentre, single-blind, randomised controlled trial. Lancet Respir. Med. 2019;7:870–880. doi: 10.1016/S2213-2600(19)30138-9. - DOI - PubMed
-
- Duggal A., Rezoagli E., Pham T., McNicholas B.A., Fan E., Bellani G., Rubenfeld G., Pesenti A.M., Laffey J.G., LUNG SAFE Investigators et al. Patterns of Use of Adjunctive Therapies in Patients with Early Moderate to Severe ARDS: Insights from the LUNG SAFE Study. Chest. 2020;157:1497–1505. doi: 10.1016/j.chest.2020.01.041. - DOI - PubMed
-
- Guérin C., Beuret P., Constantin J.M., Bellani G., Garcia-Olivares P., Roca O., Meertens J.H., Maia P.A., Becher T., Peterson J., et al. A prospective international observational prevalence study on prone positioning of ARDS patients: The APRONET (ARDS Prone Position Network) study. Intensive Care Med. 2018;44:22–37. doi: 10.1007/s00134-017-4996-5. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
