

The Vessels-Bone Axis: Iliac Artery Calcifications, Vertebral Fractures and Vitamin K from VIKI Study
- PMID: 34684568
- PMCID: PMC8539275
- DOI: 10.3390/nu13103567
The Vessels-Bone Axis: Iliac Artery Calcifications, Vertebral Fractures and Vitamin K from VIKI Study
Abstract
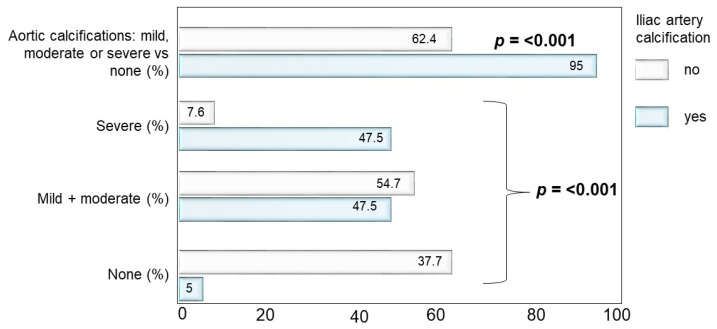
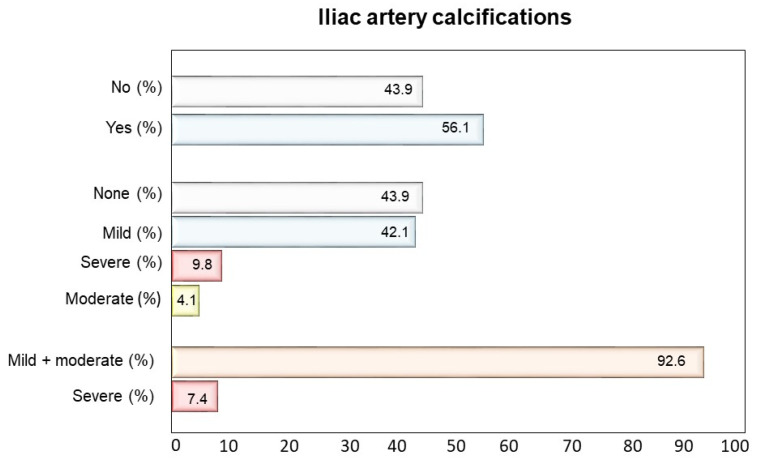
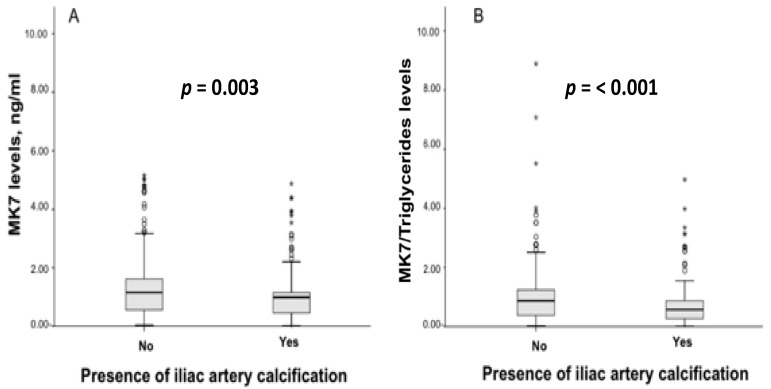
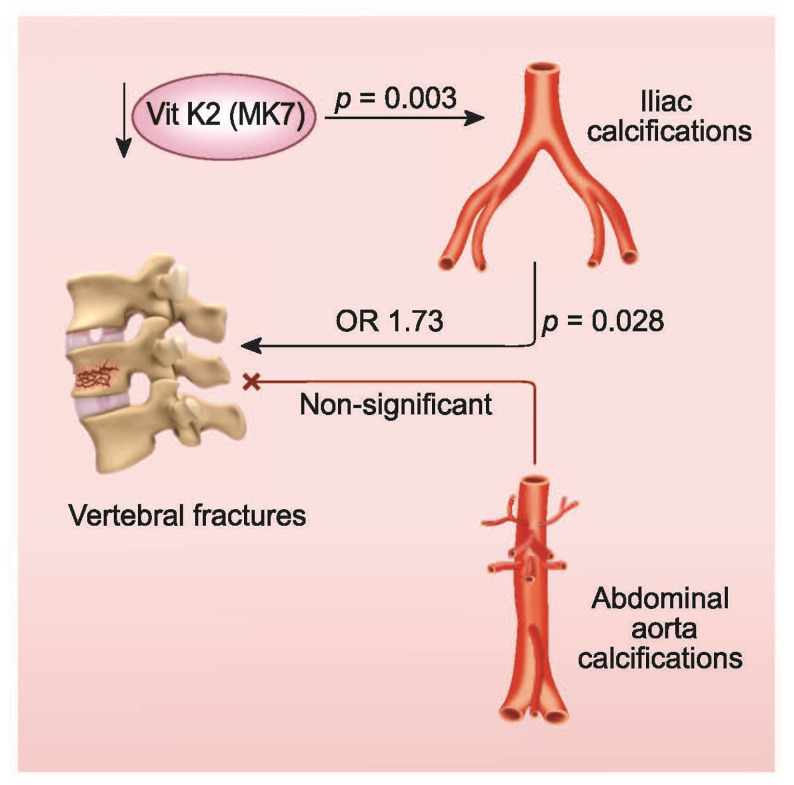
Vascular calcification and fragility fractures are associated with high morbidity and mortality, especially in end-stage renal disease. We evaluated the relationship of iliac arteries calcifications (IACs) and abdominal aortic calcifications (AACs) with the risk for vertebral fractures (VFs) in hemodialysis patients. The VIKI study was a multicenter cross-sectional study involving 387 hemodialysis patients. The biochemical data included bone health markers, such as vitamin K levels, vitamin K-dependent proteins, vitamin 25(OH)D, alkaline phosphatase, parathormone, calcium, and phosphate. VF, IACs and AACs was determined through standardized spine radiograms. VF was defined as >20% reduction of vertebral body height, and VC were quantified by measuring the length of calcium deposits along the arteries. The prevalence of IACs and AACs were 56.1% and 80.6%, respectively. After adjusting for confounding variables, the presence of IACs was associated with 73% higher odds of VF (p = 0.028), whereas we found no association (p = 0.294) for AACs. IACs were associated with VF irrespective of calcification severity. Patients with IACs had lower levels of vitamin K2 and menaquinone 7 (0.99 vs. 1.15 ng/mL; p = 0.003), and this deficiency became greater with adjustment for triglycerides (0.57 vs. 0.87 ng/mL; p < 0.001). IACs, regardless of their extent, are a clinically relevant risk factor for VFs. The association is enhanced by adjusting for vitamin K, a main player in bone and vascular health. To our knowledge these results are the first in the literature. Prospective studies are needed to confirm these findings both in chronic kidney disease and in the general population.
Keywords: epidemiology; metabolic syndrome; peripheral vascular disease; vitamin K.
Conflict of interest statement
The authors declare no conflict of interest as to the study content.
Figures
References
-
- Arboleya L., Díaz-Curiel M., Del Río L., Blanch J., Díez-Pérez A., Guañabens N., Quesada J.M., Sosa M., Gómez C., Muñoz-Torres M., et al. Prevalence of vertebral fracture in postmenopausal women with lumbar osteopenia using MorphoXpressSR (OSTEOXPRESS Study) Aging Clin. Exp. Res. 2010;22:419–426. doi: 10.1007/BF03337737. - DOI - PubMed
