

Reduction of Major Adverse Cardiovascular Events (MACE) after Bariatric Surgery in Patients with Obesity and Cardiovascular Diseases: A Systematic Review and Meta-Analysis
- PMID: 34684569
- PMCID: PMC8537443
- DOI: 10.3390/nu13103568
Reduction of Major Adverse Cardiovascular Events (MACE) after Bariatric Surgery in Patients with Obesity and Cardiovascular Diseases: A Systematic Review and Meta-Analysis
Abstract
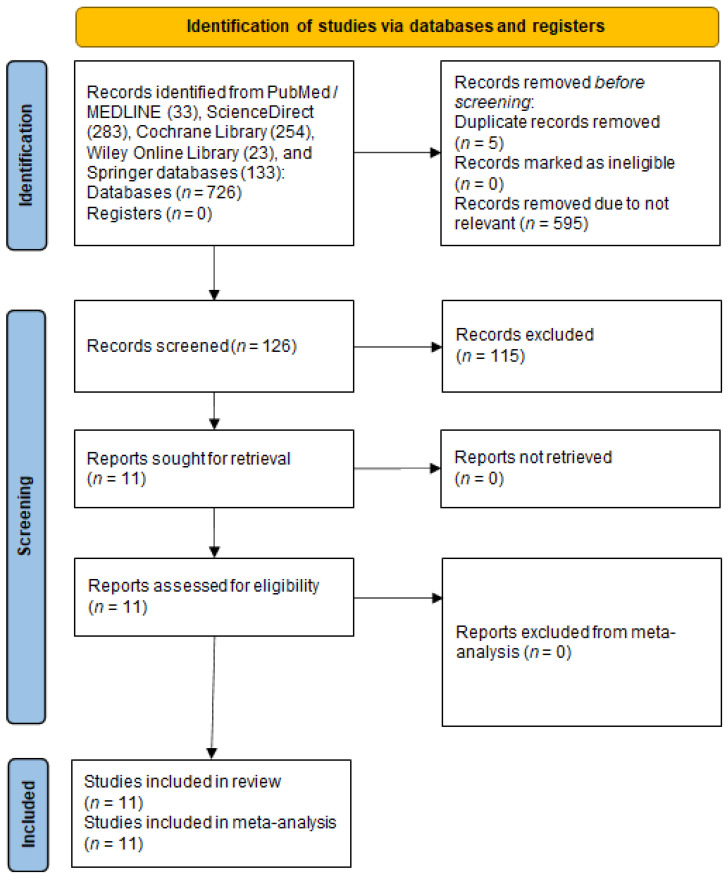
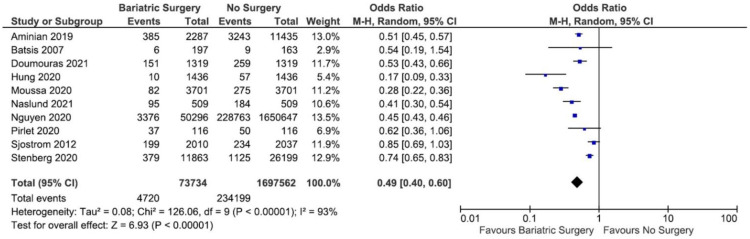
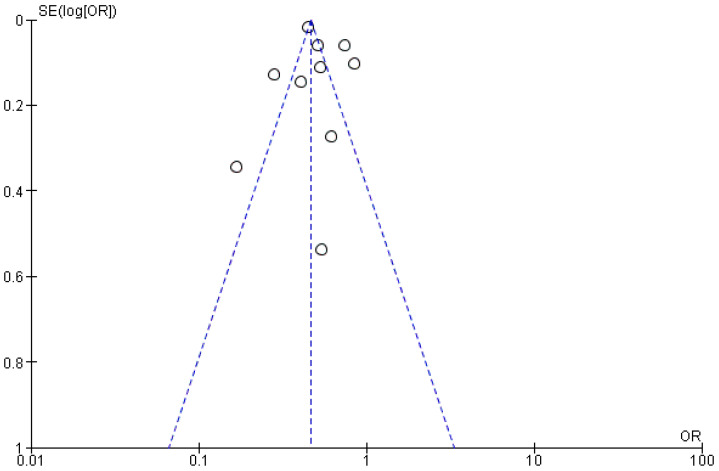
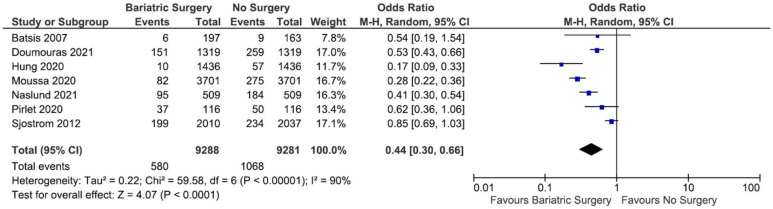
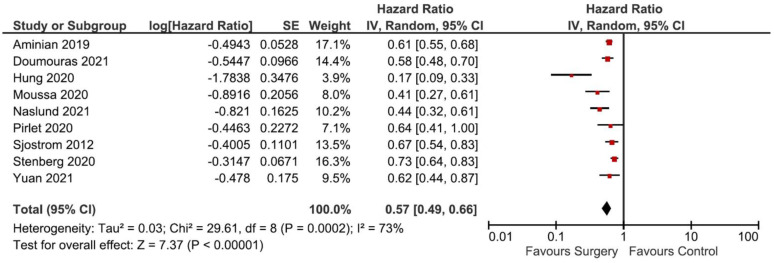
Cardiovascular diseases (CVDs) are the leading cause of death worldwide and obesity is a major risk factor that increases the morbidity and mortality of CVDs. Lifestyle modifications (e.g., diet control, physical exercise and behavioral changes) have been the first-line managements of obesity for decades. Nonetheless, when such interventions fail, pharmacotherapies and bariatric surgery are considered. Interestingly, a sudden weight loss (e.g., due to bariatric surgery) could also increase mortality. Thus, it remains unclear whether the bariatric surgery-associated weight reduction in patients with obesity and CVDs is beneficial for the reduction of Major Adverse Cardiovascular Events (MACE). Here, we performed a systematic literature search and meta-analysis of published studies comparing MACE in patients with obesity and CVDs who underwent bariatric surgery with control patients (no surgery). Eleven studies, with a total of 1,772,305 patients, which consisted of 74,042 patients who underwent any form of bariatric surgery and 1,698,263 patients with no surgery, were included in the systematic review. Next, the studies' data, including odds ratio (OR) and adjusted hazard ratio (aHR), were pooled and analyzed in a meta-analysis using a random effect model. The meta-analysis of ten studies showed that the bariatric surgery group had significantly lower odds of MACE as compared to no surgery (OR = 0.49; 95% CI 0.40-0.60; p < 0.00001; I2 = 93%) and the adjustment to confounding variables in nine studies revealed consistent results (aHR = 0.57; 95% CI 0.49-0.66; p < 0.00001; I2 = 73%), suggesting the benefit of bariatric surgery in reducing the occurrence of MACE in patients with obesity and CVDs (PROSPERO ID: CRD42021274343).
Keywords: bariatric surgery; cardiovascular disease; major adverse cardiovascular events; meta-analysis; obesity; risk factor; systematic review; weight intervention.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Roth G.A., Mensah G.A., Johnson C.O., Addolorato G., Ammirati E., Baddour L.M., Barengo N.C., Beaton A.Z., Benjamin E.J., Benziger C.P., et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010. - DOI - PMC - PubMed
-
- Powell-Wiley T.M., Poirier P., Burke L.E., Despres J.P., Gordon-Larsen P., Lavie C.J., Lear S.A., Ndumele C.E., Neeland I.J., Sanders P., et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2021;143:e984–e1010. doi: 10.1161/CIR.0000000000000973. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
