

Outcomes post fragility fracture among members of an integrated healthcare organization
- PMID: 34686906
- PMCID: PMC8930877
- DOI: 10.1007/s00198-021-06205-w
Outcomes post fragility fracture among members of an integrated healthcare organization
Abstract
This study highlights an unmet need in osteoporosis management, suggesting that beyond bone mineral density and fracture history, gender, fracture type, and age should be considered for fracture risk assessment. Following fragility fracture, men, patients with a spine or hip fracture, and those aged ≥ 65 have a higher disease burden.
Introduction: The objective of this study was to characterize osteoporosis-related fracture incidence and identify predictors of subsequent fractures and mortality.
Methods: This retrospective cohort study, conducted within Kaiser Permanente Southern California, included patients aged ≥ 50 years with qualifying fractures from 1/1/2007 to 12/31/2016, identified from diagnosis/procedure codes. Rates for fracture incidence, mortality, and resource utilization in the year post-fracture are reported. Associations between index fracture types and demographic/clinical characteristics, and mortality, subsequent fracture, and rehospitalization outcomes were estimated.
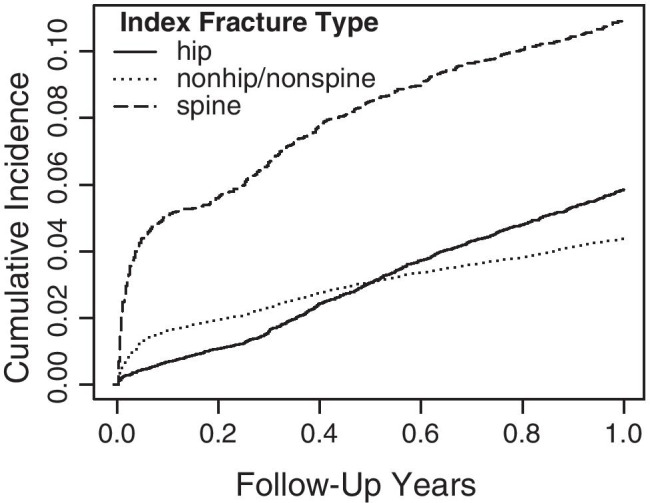
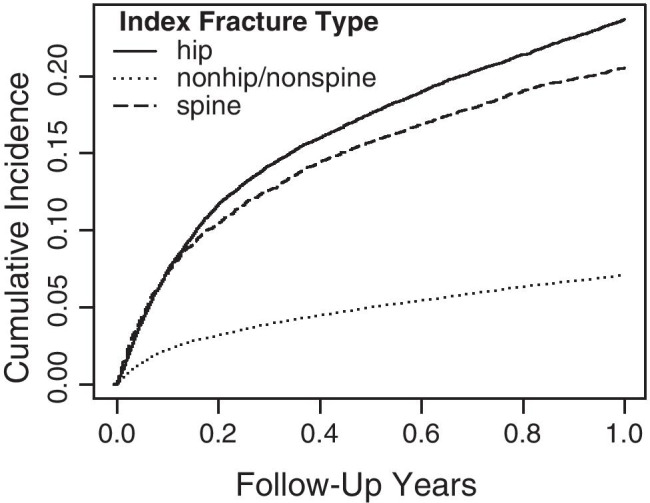
Results: Of 63,755 eligible patients, 66.7% were ≥ 65 years and 69.1% female. Index fractures included nonhip/nonspine (64.4%), hip (25.3%), and spine (10.3%). Age-adjusted subsequent fracture rate/100 person-years was higher for those with an index spine (14.5) versus hip fracture (6.3). Hospitalization rate/100 person-years was highest for patients ≥ 65 (31.8) and for spine fractures (43.5). Men (vs women) had higher age-adjusted rates of hospitalization (19.4; 17.7), emergency room visits (73.8; 66.3), and use of rehabilitation services (31.7; 27.2). The 30-day age-adjusted mortality rate/100 person-years was 46.7, 32.4, and 15.5 for spine, hip, and nonspine/nonhip fractures. The 1-year age-adjusted mortality rate/100 person-years was 14.7 for spine and 15.6 for hip fractures. In multivariable analyses, spine and hip fractures (vs nonhip/nonspine fractures) were significant predictors of 1-year mortality, all-cause and osteoporosis-related hospitalization, and nursing home use (all P-values < 0.0001).
Conclusion: Morbidity is high in the year following a fragility fracture and men, patients with a spine or hip fracture, and those aged ≥ 65 have a greater disease burden.
Keywords: Fracture risk; Mortality; Osteoporosis; Subsequent fracture.
© 2021. The Author(s).
Conflict of interest statement
Financial: Annette L. Adams is an employee of Kaiser Permanente which received funding from Radius Health, Inc. to conduct the study. Denison S. Ryan is an employee of Kaiser Permanente which received funding from Radius Health, Inc. to conduct the study. Bonnie H. Li is an employee of Kaiser Permanente which received funding from Radius Health, Inc. to conduct the study. Setareh A. Williams is an employee and shareholder of Radius Health, Inc. Yamei Wang is an employee and shareholder of Radius Health, Inc. Richard J. Weiss is a former employee and shareholder of Radius Health, Inc. Dennis M. Black provided consultancy for EffRx Pharmaceuticals, received research funding from Radius Health, Inc., and is on a data safety monitoring board for Eli Lilly (non-bone related).
Personal: The authors declare that they have no personal conflicts.
Figures
Similar articles
-
Utilization of DXA Bone Mineral Densitometry in Ontario: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(20):1-180. Epub 2006 Nov 1. Ont Health Technol Assess Ser. 2006. PMID: 23074491 Free PMC article.
-
Non-hip, non-spine fractures drive healthcare utilization following a fracture: the Global Longitudinal Study of Osteoporosis in Women (GLOW).Osteoporos Int. 2013 Jan;24(1):59-67. doi: 10.1007/s00198-012-1968-z. Epub 2012 Apr 12. Osteoporos Int. 2013. PMID: 22525976 Free PMC article.
-
A survey of outcomes and management of patients post fragility fractures in China.Osteoporos Int. 2015 Nov;26(11):2631-40. doi: 10.1007/s00198-015-3162-6. Epub 2015 May 13. Osteoporos Int. 2015. PMID: 25966892
-
Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA).Arch Osteoporos. 2013;8(1):136. doi: 10.1007/s11657-013-0136-1. Epub 2013 Oct 11. Arch Osteoporos. 2013. PMID: 24113837 Free PMC article. Review.
-
Osteoporosis in the European Union: a compendium of country-specific reports.Arch Osteoporos. 2013;8(1):137. doi: 10.1007/s11657-013-0137-0. Epub 2013 Oct 11. Arch Osteoporos. 2013. PMID: 24113838 Free PMC article. Review.
Cited by
-
Hidden blood loss and its risk factors in percutaneous vertebroplasty surgery for osteoporotic vertebral compression fractures.Arch Orthop Trauma Surg. 2023 Sep;143(9):5575-5581. doi: 10.1007/s00402-023-04873-3. Epub 2023 Apr 8. Arch Orthop Trauma Surg. 2023. PMID: 37029796
-
Refracture and mortality risk in the elderly with osteoporotic fractures: the AGES-Reykjavik study.Osteoporos Int. 2024 Jul;35(7):1231-1241. doi: 10.1007/s00198-024-07096-3. Epub 2024 Apr 24. Osteoporos Int. 2024. PMID: 38658459 Free PMC article.
-
Achieving osteoporosis treat-to-target goals with teriparatide or alendronate: sub-analysis of Japanese Osteoporosis Intervention Trial-05 (JOINT-05).J Bone Miner Metab. 2024 May;42(3):382-388. doi: 10.1007/s00774-024-01515-5. Epub 2024 May 16. J Bone Miner Metab. 2024. PMID: 38755328 Free PMC article. Clinical Trial.
-
Global, regional, national trends of femur fracture and machine learning prediction: Comprehensive findings and questions from global burden of disease 1990-2019.J Orthop Translat. 2024 May 17;46:46-52. doi: 10.1016/j.jot.2024.03.002. eCollection 2024 May. J Orthop Translat. 2024. PMID: 38800094 Free PMC article.
-
Osteoporosis management and secondary fragility fracture rates in patients with multiple sclerosis: a matched cohort study.Osteoporos Int. 2022 Sep;33(9):1999-2010. doi: 10.1007/s00198-022-06451-6. Epub 2022 Jun 7. Osteoporos Int. 2022. PMID: 35670832
References
-
- Dempster DW. Osteoporosis and the burden of osteoporosis-related fractures. Am J Manag Care. 2011;17:S164–169. - PubMed
