

COVID-19 Vaccine Response in People with Multiple Sclerosis
- PMID: 34687063
- PMCID: PMC8652739
- DOI: 10.1002/ana.26251
COVID-19 Vaccine Response in People with Multiple Sclerosis
Abstract
Objective: The purpose of this study was to investigate the effect of disease modifying therapies on immune response to severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) vaccines in people with multiple sclerosis (MS).
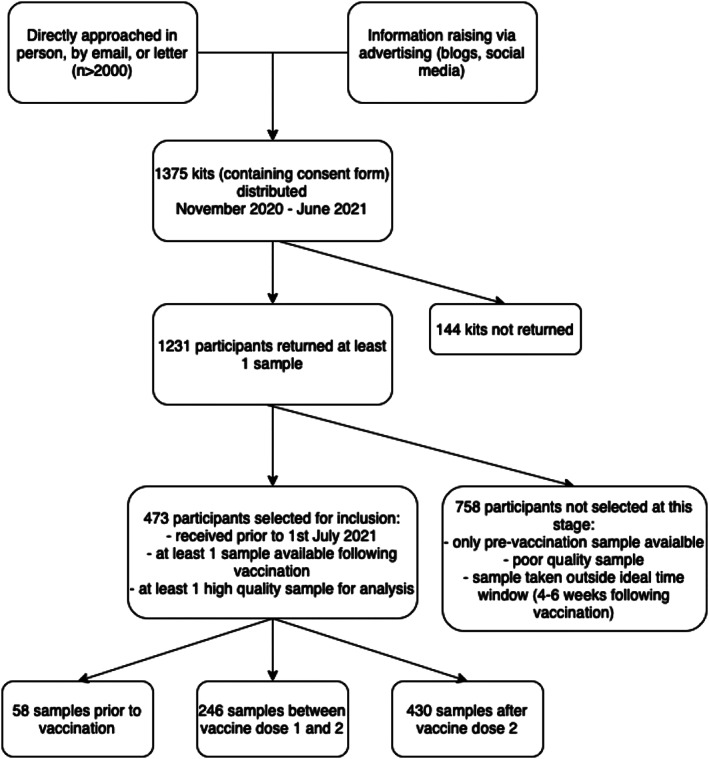
Methods: Four hundred seventy-three people with MS provided one or more dried blood spot samples. Information about coronavirus disease 2019 (COVID-19) and vaccine history, medical, and drug history were extracted from questionnaires and medical records. Dried blood spots were eluted and tested for antibodies to SARS-CoV-2. Antibody titers were partitioned into tertiles with people on no disease modifying therapy as a reference. We calculated the odds ratio of seroconversion (univariate logistic regression) and compared quantitative vaccine response (Kruskal Wallis) following the SARS-CoV-2 vaccine according to disease modifying therapy. We used regression modeling to explore the effect of vaccine timing, treatment duration, age, vaccine type, and lymphocyte count on vaccine response.
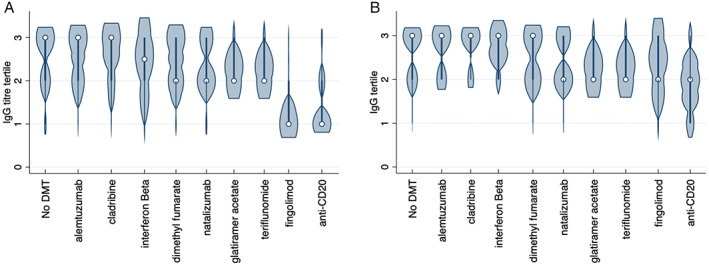
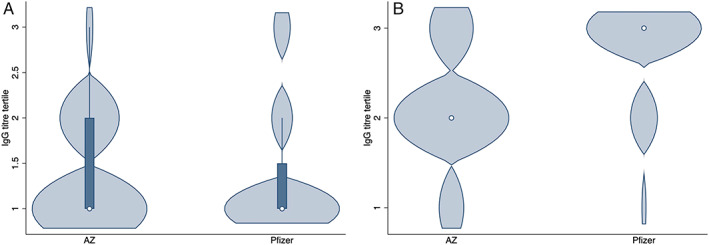
Results: Compared to no disease modifying therapy, the use of anti-CD20 monoclonal antibodies (odds ratio = 0.03, 95% confidence interval [CI] = 0.01-0.06, p < 0.001) and fingolimod (odds ratio = 0.04; 95% CI = 0.01-0.12) were associated with lower seroconversion following the SARS-CoV-2 vaccine. All other drugs did not differ significantly from the untreated cohort. Both time since last anti-CD20 treatment and total time on treatment were significantly associated with the response to the vaccination. The vaccine type significantly predicted seroconversion, but not in those on anti-CD20 medications. Preliminary data on cellular T-cell immunity showed 40% of seronegative subjects had measurable anti-SARS-CoV-2 T cell responses.
Interpretation: Some disease modifying therapies convey risk of attenuated serological response to SARS-CoV-2 vaccination in people with MS. We provide recommendations for the practical management of this patient group. ANN NEUROL 20219999:n/a-n/a.
© 2021 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Biogen, Merck, Novartis, Roche, Sanofi/Genzyme, and Teva all manufacture multiple sclerosis disease modifying therapies that were used in this study, or which could be affected by the study. The following authors have received speaker fees, consultancy fees, and/ or travel expenses to attend educational meetings from one or more of these companies: E.C.T., D.B., R.D., N.E., G.G., A.K., N.P.R., K.S., S.J., M.J.S., and A.G. are co‐founders of and holds equity in ImmunoServ Ltd., which provided T‐cell analysis. N.V., V.A., A.N.A., J.B., K.B., R.C., K.G., L.G., A.G., K.E.H., A.H., G.I., M.J., A.S.K., S.L., S.J.M., S.N.S., J.S., M.U., and M.W. have no conflicts of interest to declare.
Figures
References
-
- Boulton C, Meiser K, David OJ, Schmouder R. Pharmacodynamic effects of steady‐state fingolimod on antibody response in healthy volunteers: a 4‐week, randomized, placebo‐controlled, parallel‐group, multiple‐dose study. J Clin Pharmacol 2012;52:1879–1890. - PubMed
-
- Department of Health and Social Care . Most vulnerable could be offered booster COVID‐19 vaccines from September. In: GOV.UK [Internet]. 30 Jun 2021. Available at: https://www.gov.uk/government/news/most-vulnerable-could-be-offered-boos.... Accessed July 13 2021.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
