

Early childhood epilepsies: epidemiology, classification, aetiology, and socio-economic determinants
- PMID: 34687210
- PMCID: PMC8557326
- DOI: 10.1093/brain/awab162
Early childhood epilepsies: epidemiology, classification, aetiology, and socio-economic determinants
Abstract
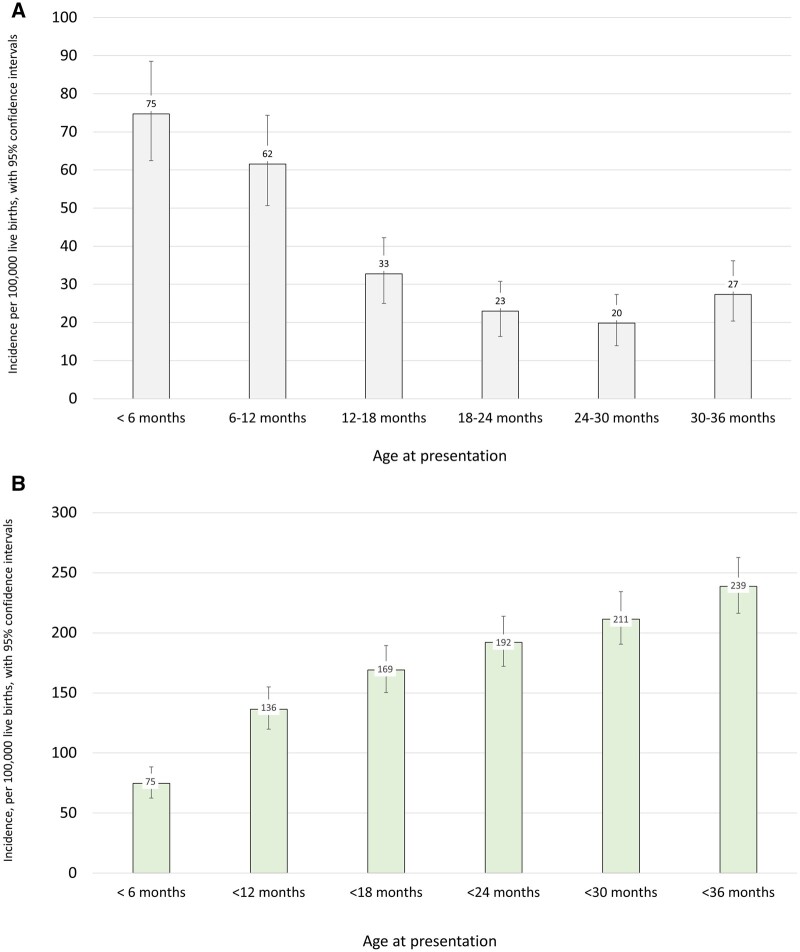
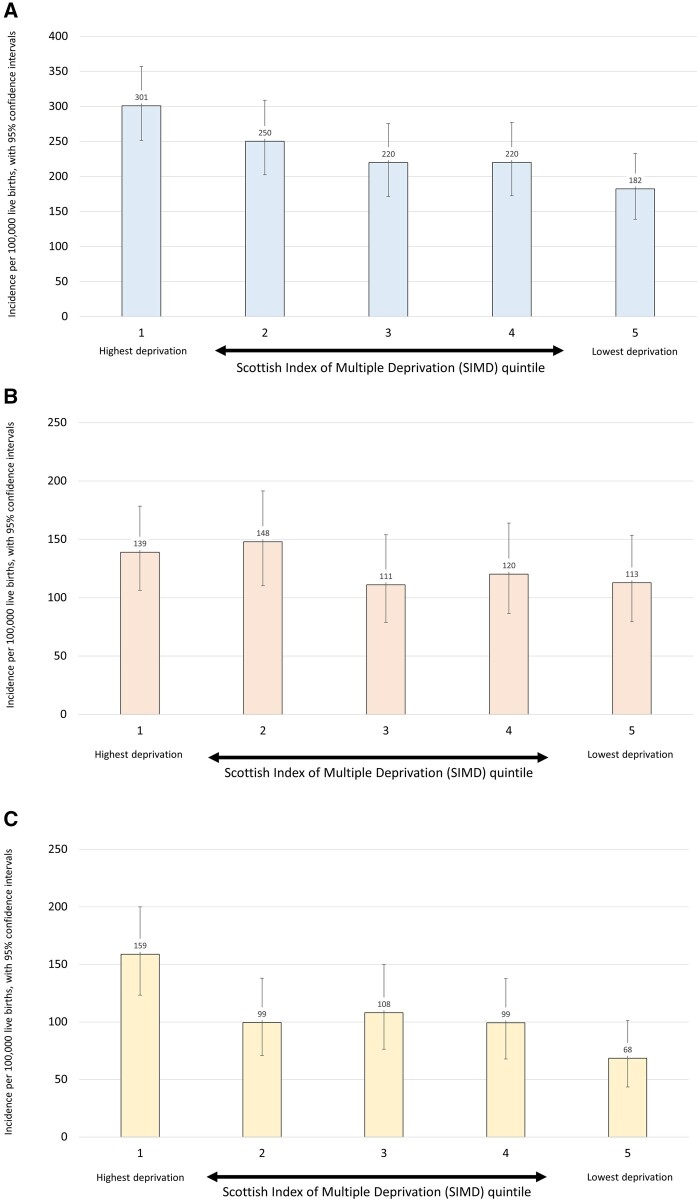
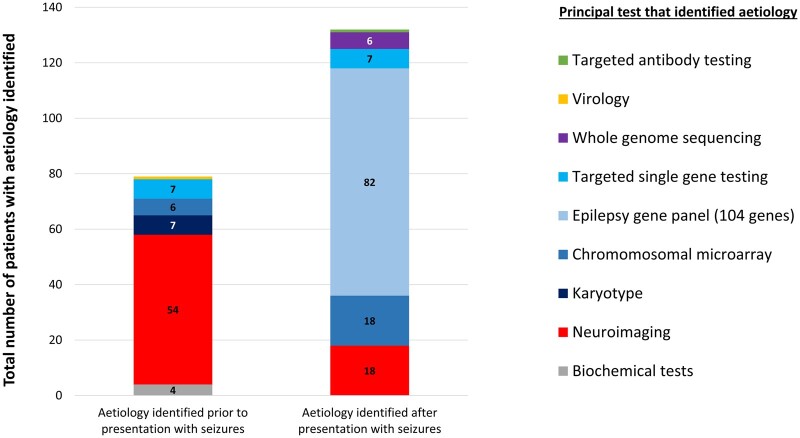
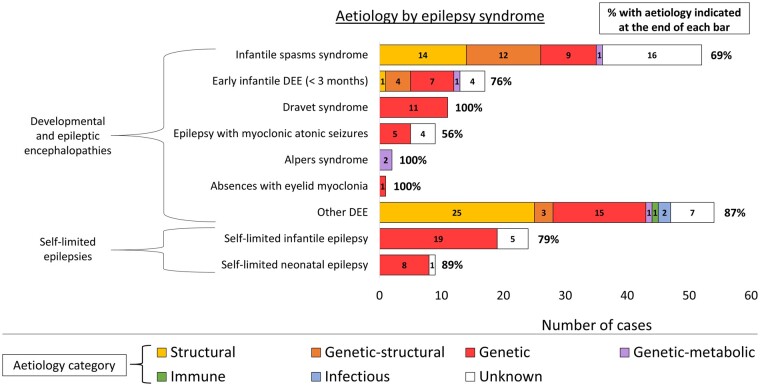
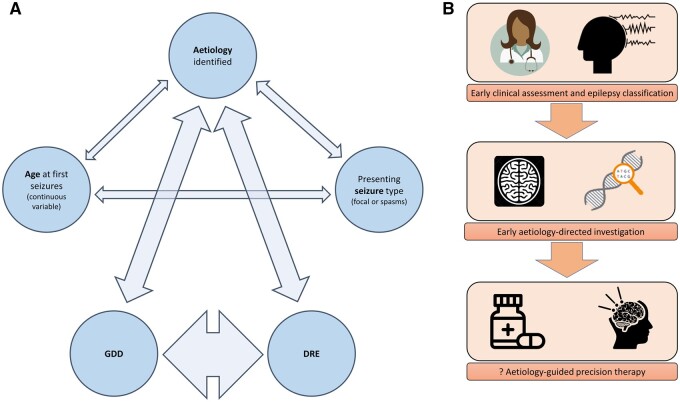
Epilepsies of early childhood are frequently resistant to therapy and often associated with cognitive and behavioural comorbidity. Aetiology focused precision medicine, notably gene-based therapies, may prevent seizures and comorbidities. Epidemiological data utilizing modern diagnostic techniques including whole genome sequencing and neuroimaging can inform diagnostic strategies and therapeutic trials. We present a 3-year, multicentre prospective cohort study, involving all children under 3 years of age in Scotland presenting with epilepsies. We used two independent sources for case identification: clinical reporting and EEG record review. Capture-recapture methodology was then used to improve the accuracy of incidence estimates. Socio-demographic and clinical details were obtained at presentation, and 24 months later. Children were extensively investigated for aetiology. Whole genome sequencing was offered for all patients with drug-resistant epilepsy for whom no aetiology could yet be identified. Multivariate logistic regression modelling was used to determine associations between clinical features, aetiology, and outcome. Three hundred and ninety children were recruited over 3 years. The adjusted incidence of epilepsies presenting in the first 3 years of life was 239 per 100 000 live births [95% confidence interval (CI) 216-263]. There was a socio-economic gradient to incidence, with a significantly higher incidence in the most deprived quintile (301 per 100 000 live births, 95% CI 251-357) compared with the least deprived quintile (182 per 100 000 live births, 95% CI 139-233), χ2 odds ratio = 1.7 (95% CI 1.3-2.2). The relationship between deprivation and incidence was only observed in the group without identified aetiology, suggesting that populations living in higher deprivation areas have greater multifactorial risk for epilepsy. Aetiology was determined in 54% of children, and epilepsy syndrome was classified in 54%. Thirty-one per cent had an identified genetic cause for their epilepsy. We present novel data on the aetiological spectrum of the most commonly presenting epilepsies of early childhood. Twenty-four months after presentation, 36% of children had drug-resistant epilepsy (DRE), and 49% had global developmental delay (GDD). Identification of an aetiology was the strongest determinant of both DRE and GDD. Aetiology was determined in 82% of those with DRE, and 75% of those with GDD. In young children with epilepsy, genetic testing should be prioritized as it has the highest yield of any investigation and is most likely to inform precision therapy and prognosis. Epilepsies in early childhood are 30% more common than previously reported. Epilepsies of undetermined aetiology present more frequently in deprived communities. This likely reflects increased multifactorial risk within these populations.
Keywords: epidemiology; epilepsy; genetics; incidence; precision.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com.
Figures
References
-
- Fisher RS, Emde V, Boas W, et al. Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia. 2005;46(4):470–472. - PubMed
-
- Fisher RS, Acevedo C, Arzimanoglou A, et al. A practical definition of epilepsy. Epilepsia. 2014;55(4):475–482. - PubMed
-
- Devinsky O, Patel AD, Cross JH, et al. ; GWPCARE3 Study Group. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N Eng J Med. 2018;378(20):1888–1897. - PubMed
-
- Thiele EA, Marsh ED, French JA, et al. Cannabidiol in a patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4): A randomised double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10125):1085–1096. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
