

Alzheimer's disease associated with Down syndrome: a genetic form of dementia
- PMID: 34687637
- PMCID: PMC9387748
- DOI: 10.1016/S1474-4422(21)00245-3
Alzheimer's disease associated with Down syndrome: a genetic form of dementia
Abstract
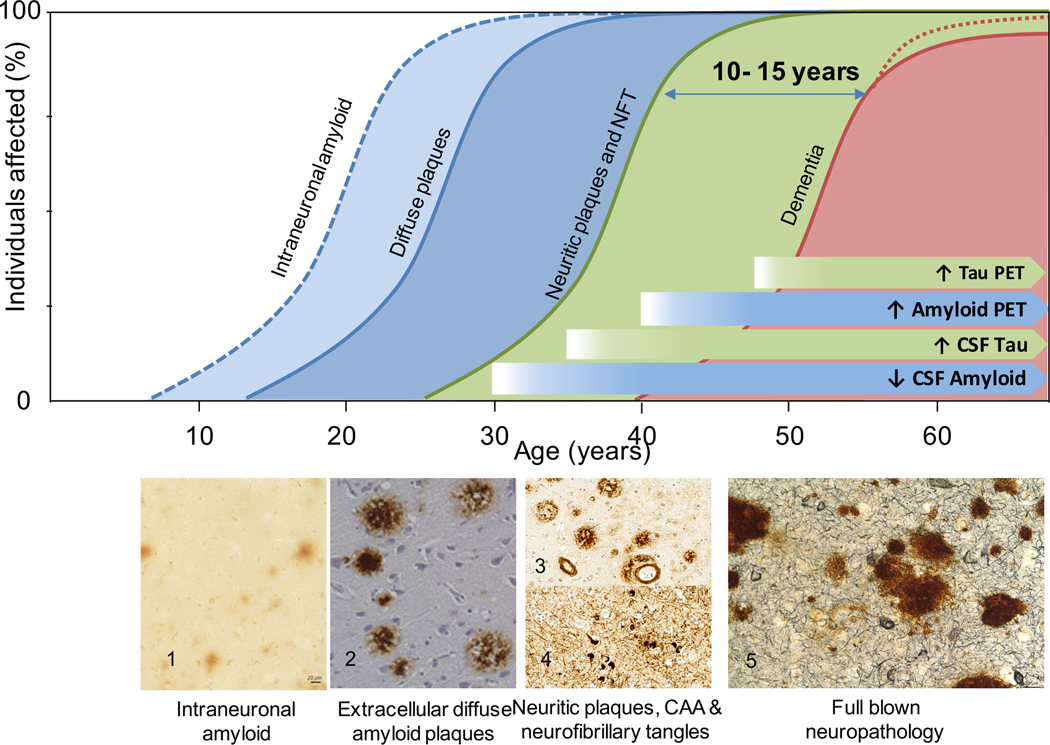
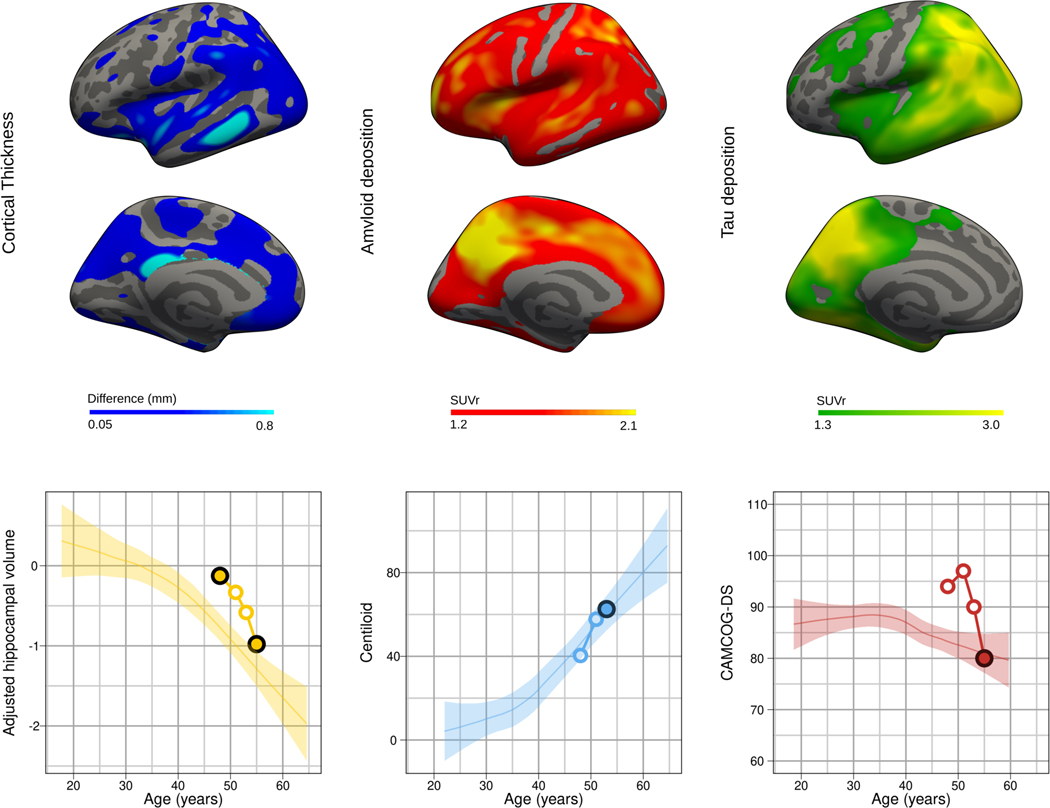
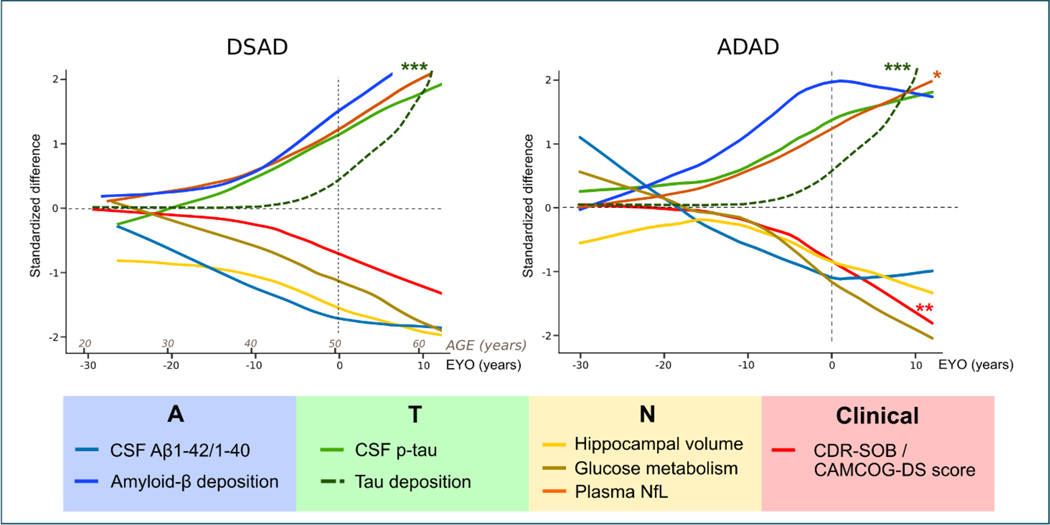
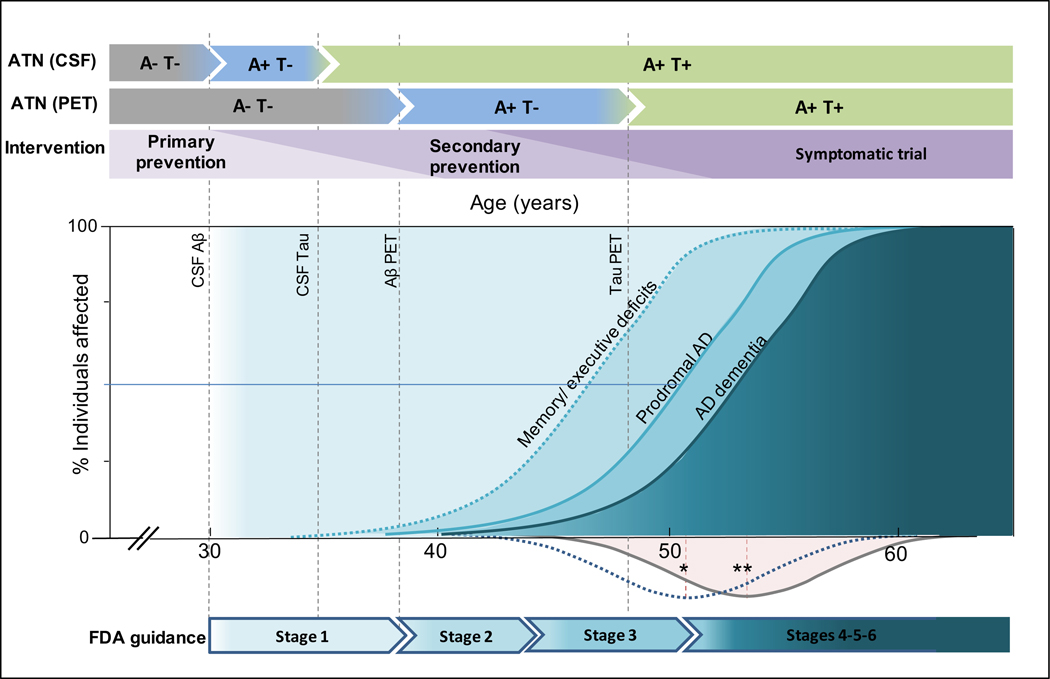
Adults with Down syndrome develop the neuropathological hallmarks of Alzheimer's disease and are at very high risk of developing early-onset dementia, which is now the leading cause of death in this population. Diagnosis of dementia remains a clinical challenge because of the lack of validated diagnostic criteria in this population, and because symptoms are overshadowed by the intellectual disability associated with Down syndrome. In people with Down syndrome, fluid and imaging biomarkers have shown good diagnostic performances and a strikingly similar temporality of changes with respect to sporadic and autosomal dominant Alzheimer's disease. Most importantly, there are no treatments to prevent Alzheimer's disease, even though adults with Down syndrome could be an optimal population in whom to conduct Alzheimer's disease prevention trials. Unprecedented research activity in Down syndrome is rapidly changing this bleak scenario that will translate into disease-modifying therapies that could benefit other populations.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests JF reports grants from the Fondo de Investigaciones Sanitario (FIS), Instituto de Salud Carlos III (PI14/01126 and PI17/01019), and the CIBERNED programme (Program 1, Alzheimer Disease and SIGNAL study, www.signalstudy.es), partly jointly funded by Fondo Europeo de Desarrollo Regional, Unión Europea, Una manera de hacer Europa. This work was also supported by the National Institutes of Health (NIH; National Institute on Aging [NIA] grants 1R01AG056850 - 01A1; R21AG056974, and R01AG061566), Fundació La Marató de TV3 (20141210), by grants from Fundació Víctor Grífols i Lucas, and by the Generalitat de Catalunya (SLT006/17/00119). JF is a consultant to Novartis and Merck, has received conference fees from Esteve, NovoNordisk, and Biogen, has been part of the AC Immune and Lundbeck advisory boards, and owns a patent (EP18382175.0). SHZ is supported by the Cambridgeshire & Peterborough NHS Foundation Trust, and is part of The Alzheimer's Biomarkers Consortium—Down Syndrome, funded by the NIA and the Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD; U01 AG051406 and U01 AG051412). SH reports grants from the NICHD core grant (NICHD U54 HD090256) to support time working on papers; and grants from the NIH (R01AG031110, U01AG051406). MSR is a consultant to AC Immune and Alzheon, and has received research support from the NIH, Avid, Baxter, Eisai, Elan, Genentech, Janssen, Lilly, Merck, and Roche. EH reports funding to support acquisition of tissue from NIH/NIA U19AG068054, NIH/NICHD R01HD064993, NIH/NIA P30AG066519, and Brightfocus grant BFF17-008; and has been a consultant for AC Immune. MC-I reports grants from the FIS, Instituto de Salud Carlos III (PI18/00335), and the CIBERNED program, Alzheimer's Association and Global Brain Health Institute (GBHI_ALZ-18-543740), Jérôme Lejeune Foundation (project 1913, Cycle 2019B), and Societat Catalana de Neurologia (Premi Beca Fundació SCN 2020). This report describes independent research and the views expressed by the authors and not necessarily those of the funders. The funders did not take part in the design and undertaking of the Review; or the decision to submit the article for publication.
Figures
References
-
- Mann DMA. The pathological association between down syndrome and Alzheimer disease. Mech Ageing Dev 1988; 43: 99–136. - PubMed
-
- McCarron M, McCallion P, Reilly E, Dunne P, Carroll R, Mulryan N. A prospective 20-year longitudinal follow-up of dementia in persons with Down syndrome. J Intellect Disabil Res 2017; 61: 843–52. - PubMed
-
- Fortea J, Carmona-Iragui M, Benejam B, et al. Plasma and CSF biomarkers for the diagnosis of Alzheimer’s disease in adults with Down syndrome: a cross-sectional study. Lancet Neurol 2018; 17: 860–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
