

Thyroid crisis caused by metastatic thyroid cancer: an autopsy case report
- PMID: 34689780
- PMCID: PMC8543858
- DOI: 10.1186/s12902-021-00875-7
Thyroid crisis caused by metastatic thyroid cancer: an autopsy case report
Abstract
Background: Thyroid crisis is a life-threatening condition in thyrotoxic patients. Although differentiated thyroid cancer is one of the causes of hyperthyroidism, reports on thyroid crisis caused by thyroid cancer are quite limited. Here, we describe a case of thyroid crisis caused by metastatic thyroid cancer.
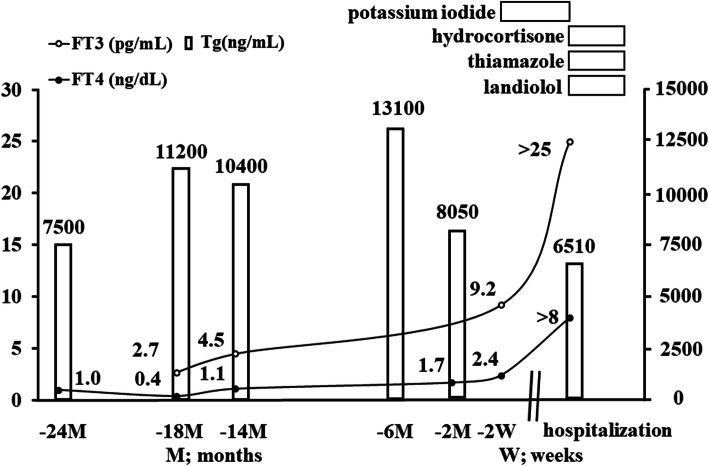
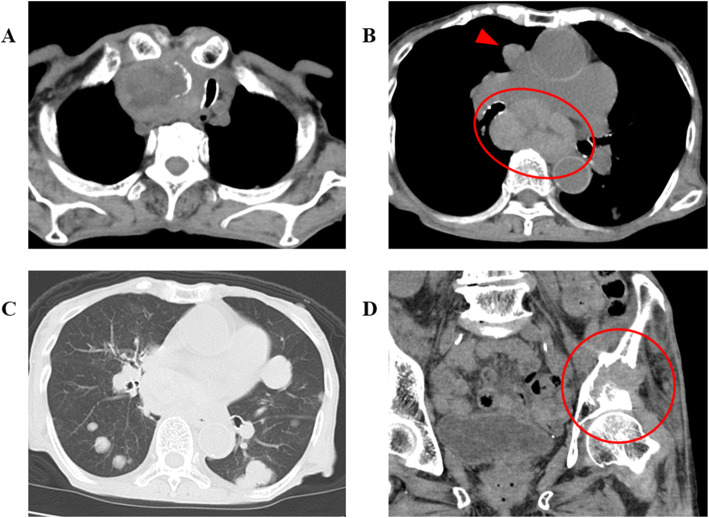
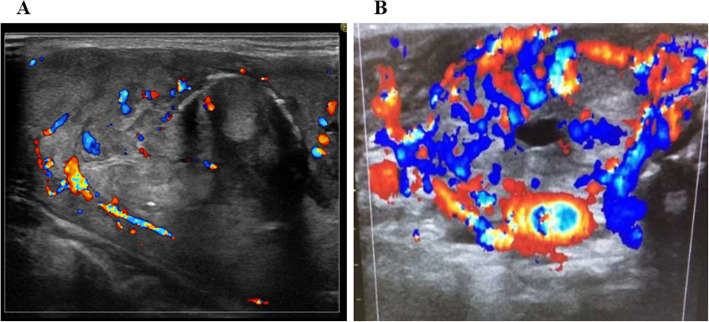
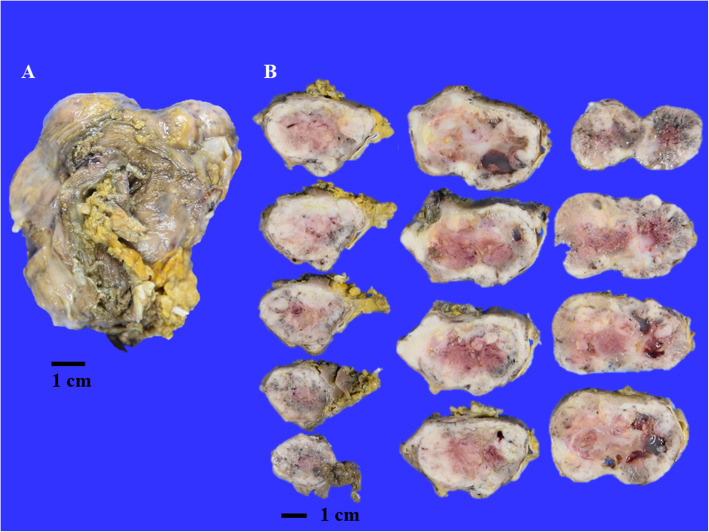
Case presentation: A 91-year-old woman was admitted to our hospital because of loss of appetite. Two years prior to this hospitalization, she presented with subclinical thyrotoxicosis and was diagnosed with histologically unidentified thyroid cancer with multiple metastases, and she refused aggressive medical interventions. On admission, she exhibited extreme thyrotoxicosis, and the presence of fever, severe tachycardia, impaired consciousness, and heart failure revealed the presence of thyroid crisis. All thyroid autoantibodies were negative. Multidisciplinary conservative treatment was initiated; however, she died on the fifth day after admission. Autopsy revealed the presence of primary anaplastic thyroid carcinoma and multiple metastatic foci arising from follicular thyroid carcinoma. Both primary and metastatic follicular thyroid carcinoma likely induced thyrotoxicosis, which could have been exacerbated by anaplastic thyroid carcinoma.
Conclusions: Even though the trigger of thyroid crisis in this patient is not clear, the aggravated progression of her clinical course suggests that careful monitoring of thyroid hormones and appropriate intervention are essential for patients with thyroid cancer.
Keywords: Anaplastic thyroid carcinoma; Follicular thyroid carcinoma; Metastasis; Thyroid crisis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests in this paper.
Figures


References
-
- Akamizu T, Satoh T, Isozaki O, Suzuki A, Wakino S, Iburi T, Tsuboi K, Monden T, Kouki T, Otani H, Teramukai S, Uehara R, Nakamura Y, Nagai M, Mori M, Japan Thyroid Association Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys. Thyroid. 2012;22(7):661–679. doi: 10.1089/thy.2011.0334. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
