

Clinical Artificial Intelligence Applications: Breast Imaging
- PMID: 34689871
- PMCID: PMC9075017
- DOI: 10.1016/j.rcl.2021.07.010
Clinical Artificial Intelligence Applications: Breast Imaging
Abstract
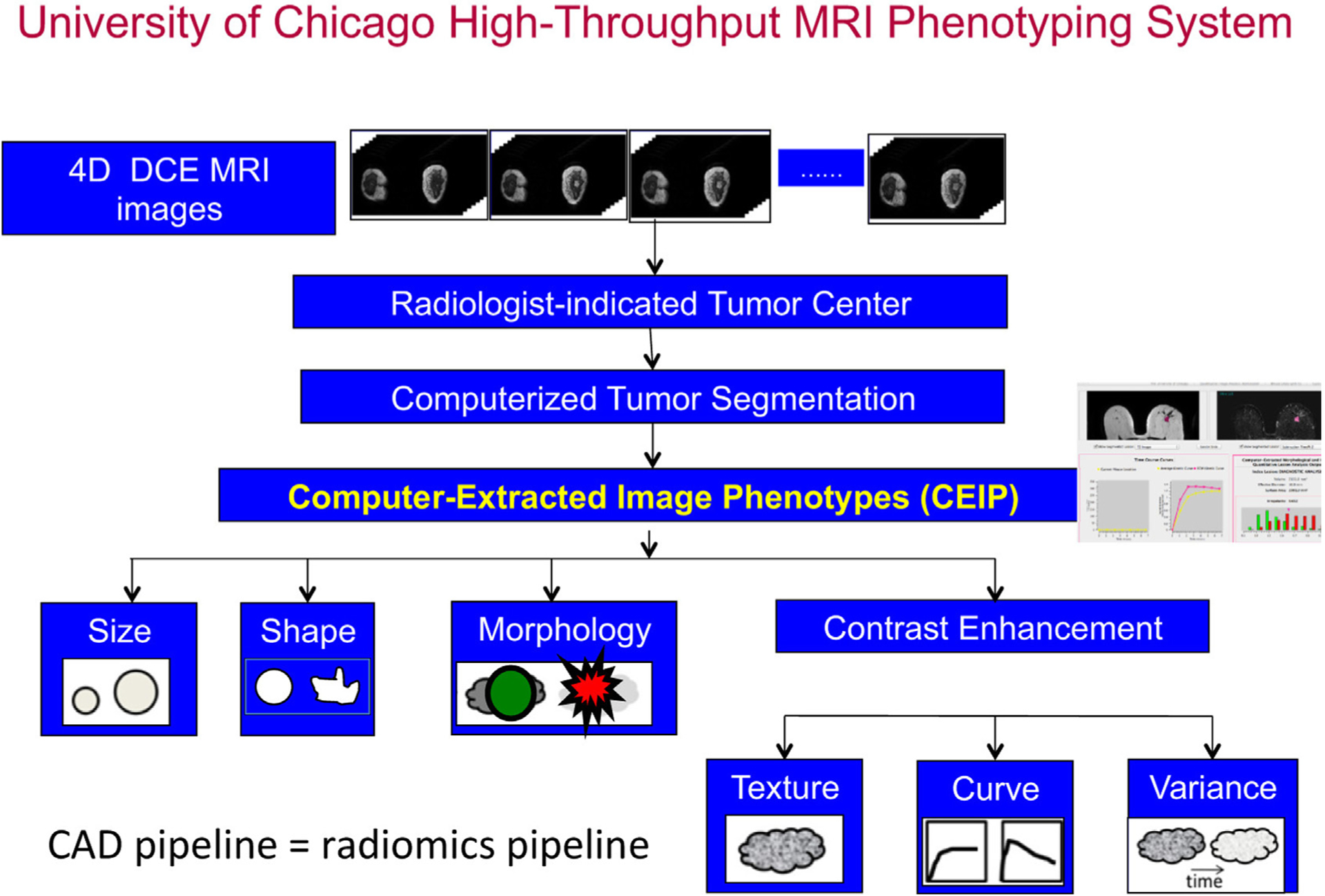
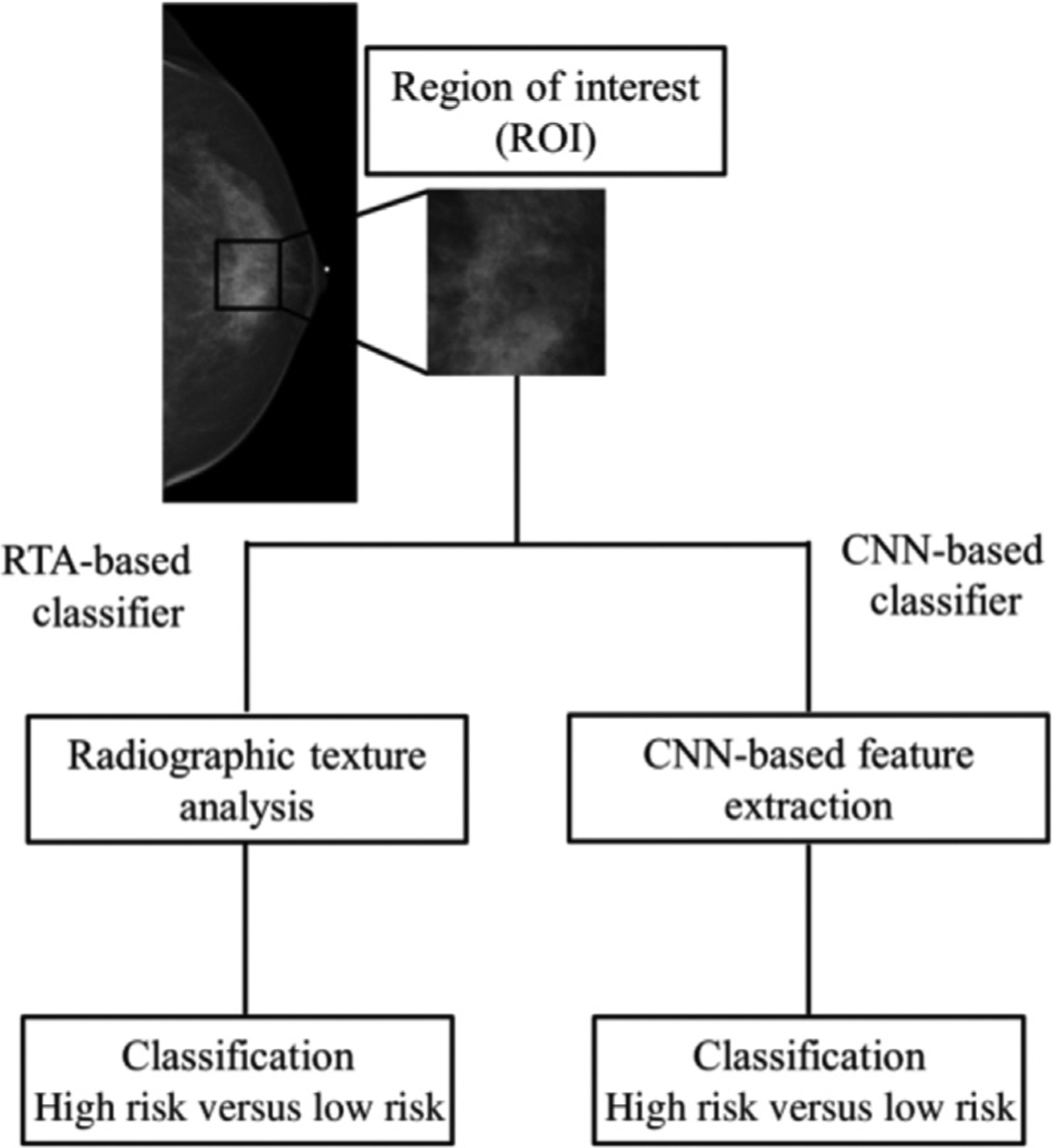
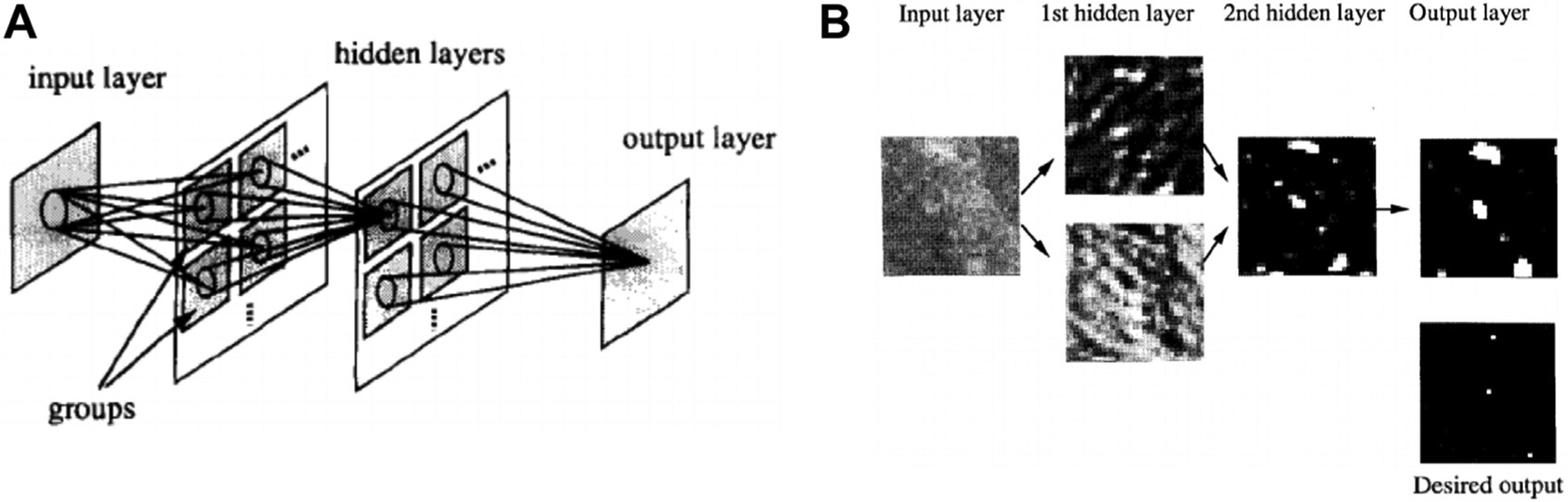
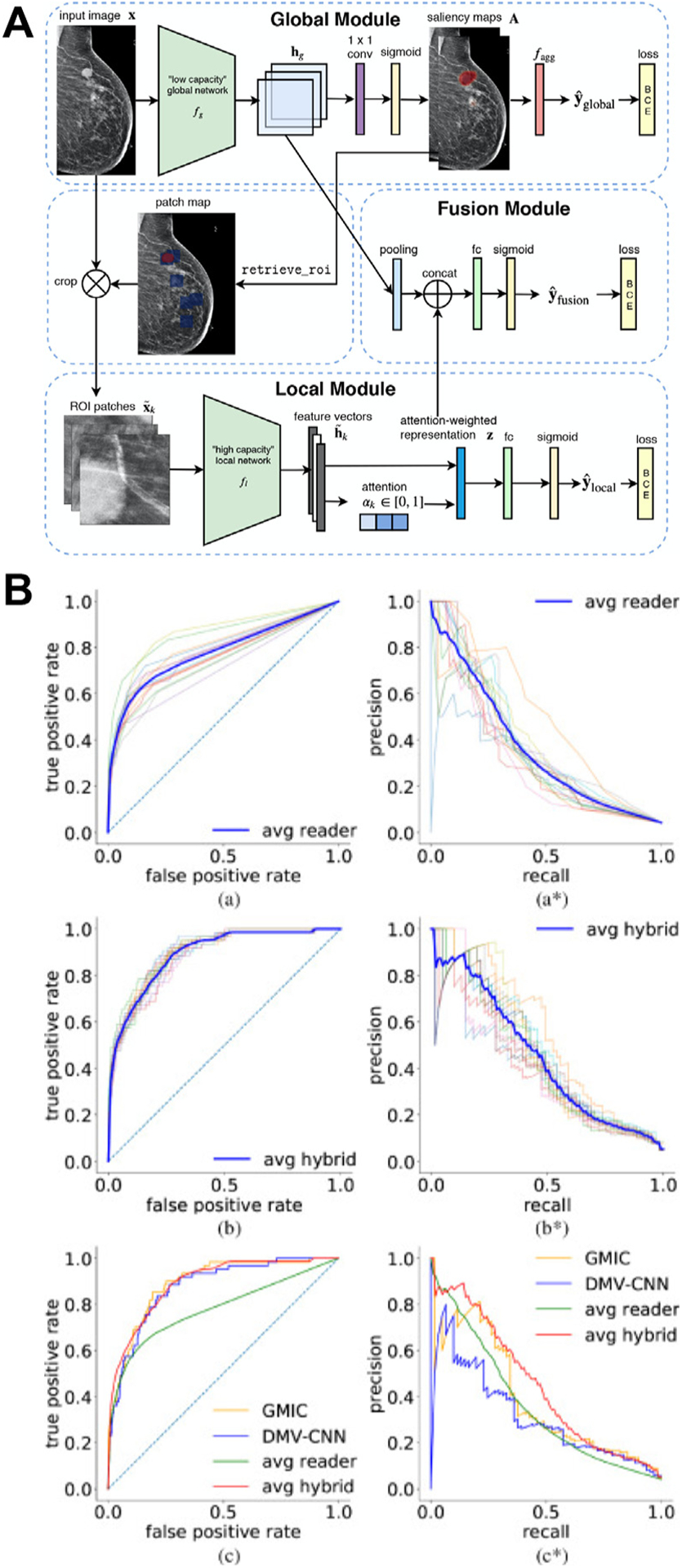
This article gives a brief overview of the development of artificial intelligence in clinical breast imaging. For multiple decades, artificial intelligence (AI) methods have been developed and translated for breast imaging tasks such as detection, diagnosis, and assessing response to therapy. As imaging modalities arise to support breast cancer screening programs and diagnostic examinations, including full-field digital mammography, breast tomosynthesis, ultrasound, and MRI, AI techniques parallel the efforts with more complex algorithms, faster computers, and larger data sets. AI methods include human-engineered radiomics algorithms and deep learning methods. Examples of these AI-supported clinical tasks are given along with commentary on the future.
Keywords: Breast cancer; Computer-aided diagnosis; Deep learning; Diagnosis; Machine learning; Medical imaging; Screening; Treatment response.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure Q.Hu declares no competing interests. M.L. Giger is a stockholder in R2 technology/Hologic and QView; receives royalties from Hologic, GE Medical Systems, MEDIAN Technologies, Riverain Medical, Mitsubishi, and Toshiba; and is a cofounder of Quantitative Insights (now Qlarity Imaging). Following the University of Chicago Conflict of Interest Policy, the investigators disclose publicly actual or potential significant financial interest that would reasonably appear to be directly and significantly affected by the research activities.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin 2021;71(1):7–33. - PubMed
-
- Niell BL, Freer PE, Weinfurtner RJ, et al. Screening for breast cancer. Radiol Clin North Am 2017;55(6): 1145–62. - PubMed
-
- ACR appropriateness criteria: breast cancer screening. American College of Radiology; 2017. Available at: https://acsearch.acr.org/docs/70910/Narrative. Accessed January 17, 2021.
-
- Mann RM, Cho N, Moy L. Breast MRI: state of the art. Radiology 2019;292(3):520–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
