

Rapid non-destructive volumetric tumor yield assessment in fresh lung core needle biopsies using polarization sensitive optical coherence tomography
- PMID: 34692203
- PMCID: PMC8515979
- DOI: 10.1364/BOE.433346
Rapid non-destructive volumetric tumor yield assessment in fresh lung core needle biopsies using polarization sensitive optical coherence tomography
Abstract
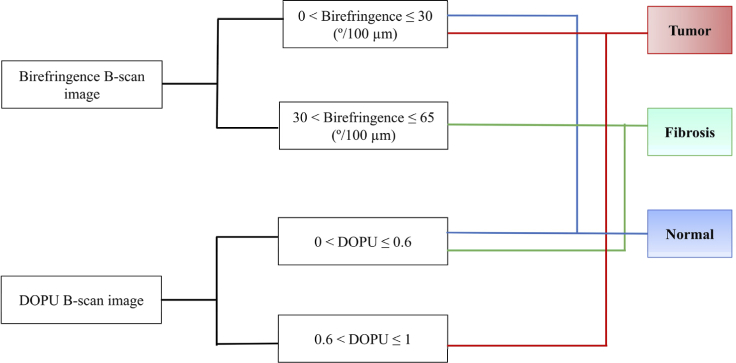
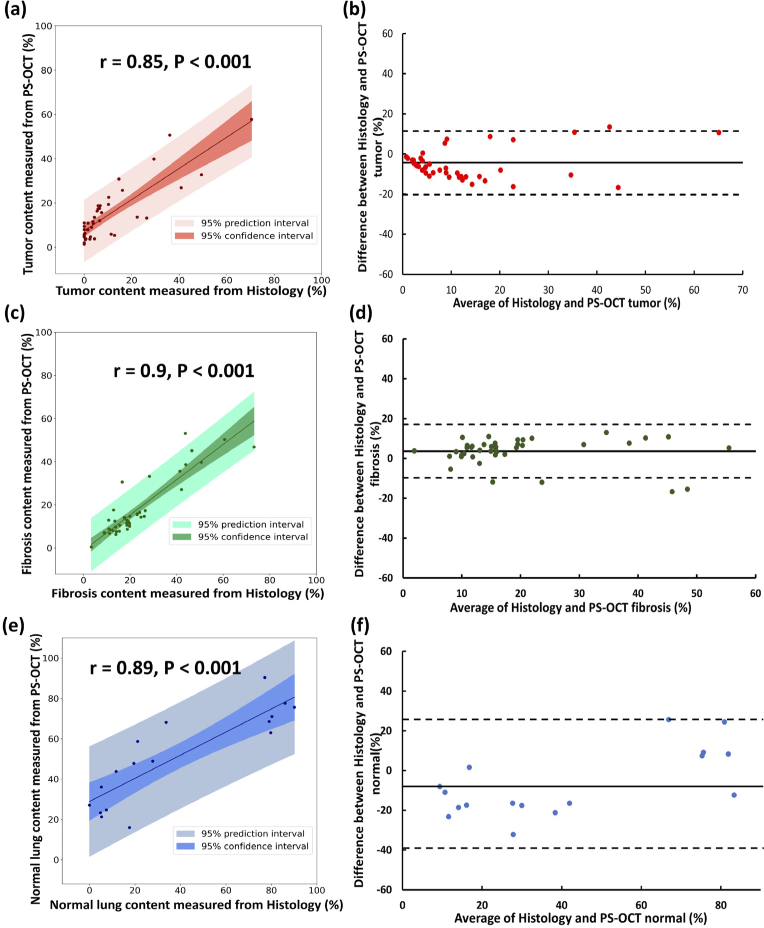
Adequate tumor yield in core-needle biopsy (CNB) specimens is essential in lung cancer for accurate histological diagnosis, molecular testing for therapeutic decision-making, and tumor biobanking for research. Insufficient tumor sampling in CNB is common, primarily due to inadvertent sampling of tumor-associated fibrosis or atelectatic lung, leading to repeat procedures and delayed diagnosis. Currently, there is no method for rapid, non-destructive intraprocedural assessment of CNBs. Polarization-sensitive optical coherence tomography (PS-OCT) is a high-resolution, volumetric imaging technique that has the potential to meet this clinical need. PS-OCT detects endogenous tissue properties, including birefringence from collagen, and degree of polarization uniformity (DOPU) indicative of tissue depolarization. Here, PS-OCT birefringence and DOPU measurements were used to quantify the amount of tumor, fibrosis, and normal lung parenchyma in 42 fresh, intact lung CNB specimens. PS-OCT results were compared to and validated against matched histology in a blinded assessment. Linear regression analysis showed strong correlations between PS-OCT and matched histology for quantification of tumors, fibrosis, and normal lung parenchyma in CNBs. PS-OCT distinguished CNBs with low tumor content from those with higher tumor content with high sensitivity and specificity. This study demonstrates the potential of PS-OCT as a method for rapid, non-destructive, label-free intra-procedural tumor yield assessment.
© 2021 Optical Society of America under the terms of the OSA Open Access Publishing Agreement.
Conflict of interest statement
LPH: Boehringer Ingelheim, Pliant Therapeutics, LX Medical, and Biogen Idec. MJS: NinePoint Medical, LX Medical.
Figures




Similar articles
-
Distinguishing Tumor from Associated Fibrosis to Increase Diagnostic Biopsy Yield with Polarization-Sensitive Optical Coherence Tomography.Clin Cancer Res. 2019 Sep 1;25(17):5242-5249. doi: 10.1158/1078-0432.CCR-19-0566. Epub 2019 Jun 7. Clin Cancer Res. 2019. PMID: 31175092 Free PMC article.
-
Determination of characteristics of degenerative joint disease using optical coherence tomography and polarization sensitive optical coherence tomography.Lasers Surg Med. 2006 Oct;38(9):852-65. doi: 10.1002/lsm.20394. Lasers Surg Med. 2006. PMID: 16998913
-
Polarization-sensitive optical coherence tomography for renal tumor detection in ex vivo human kidneys.Opt Lasers Eng. 2024 Feb;173:107900. doi: 10.1016/j.optlaseng.2023.107900. Epub 2023 Oct 23. Opt Lasers Eng. 2024. PMID: 37982078 Free PMC article.
-
In vivo polarisation sensitive optical coherence tomography for fibrosis assessment in interstitial lung disease: a prospective, exploratory, observational study.BMJ Open Respir Res. 2023 Aug;10(1):e001628. doi: 10.1136/bmjresp-2023-001628. BMJ Open Respir Res. 2023. PMID: 37553184 Free PMC article.
-
Investigating the depolarization property of skin tissue by degree of polarization uniformity contrast using polarization-sensitive optical coherence tomography.Biomed Opt Express. 2021 Jul 20;12(8):5073-5088. doi: 10.1364/BOE.424709. eCollection 2021 Aug 1. Biomed Opt Express. 2021. PMID: 34513243 Free PMC article.
Cited by
-
Digital calibration method to enable depth-resolved all-fiber polarization sensitive optical coherence tomography with an arbitrary input polarization state.Biomed Opt Express. 2024 Apr 24;15(5):3329-3343. doi: 10.1364/BOE.517826. eCollection 2024 May 1. Biomed Opt Express. 2024. PMID: 38855689 Free PMC article.
-
Reply to Kalverda et al.: Endobronchial Optical Coherence Tomography: Shining New Light on Diagnosing Usual Interstitial Pneumonitis?Am J Respir Crit Care Med. 2022 Apr 15;205(8):968-971. doi: 10.1164/rccm.202112-2737LE. Am J Respir Crit Care Med. 2022. PMID: 35148493 Free PMC article. No abstract available.
-
Advances in early detection of non-small cell lung cancer: A comprehensive review.Cancer Med. 2024 Sep;13(18):e70156. doi: 10.1002/cam4.70156. Cancer Med. 2024. PMID: 39300939 Free PMC article. Review.
-
Research progress on the application of optical coherence tomography in the field of oncology.Front Oncol. 2022 Jul 25;12:953934. doi: 10.3389/fonc.2022.953934. eCollection 2022. Front Oncol. 2022. PMID: 35957903 Free PMC article. Review.
-
Microscopic Small Airway Abnormalities Identified in Early Idiopathic Pulmonary Fibrosis In Vivo Using Endobronchial Optical Coherence Tomography.Am J Respir Crit Care Med. 2024 Aug 15;210(4):473-483. doi: 10.1164/rccm.202401-0249OC. Am J Respir Crit Care Med. 2024. PMID: 38747674 Free PMC article.
References
-
- National Lung Screening Trial Research Team , Aberle D. R., Adams A. M., Berg C. D., Black W. C., Clapp J. D., Fagerstrom R. M., Gareen I. F., Gatsonis C., Marcus P. M., Sicks J. D., “Reduced lung-cancer mortality with low-dose computed tomographic screening,” N. Engl. J. Med. 365(5):395–409 (2011).10.1056/NEJMoa1102873 - DOI - PMC - PubMed
-
- Bach P. B., Mirkin J. N., Oliver T. K., Azzoli C. G., Berry D. A., Brawley O. W., Byers T., Colditz G. A., Gould M. K., Jett J. R., Sabichi A. L.., Smith-Bindman R.., Wood D. E, Qaseem A., Detterbeck F. C., “Benefits and harms of CT screening for lung cancer: a systematic review,” JAMA 307(22), 2418–2429 (2012).10.1001/jama.2012.5521 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources