

24-h-Ambulatory Blood Pressure Monitoring in Sub-Saharan Africa: Hypertension Phenotypes and Dipping Patterns in Malawian HIV+ Patients on Antiretroviral Therapy
- PMID: 34692392
- PMCID: PMC8516010
- DOI: 10.5334/gh.945
24-h-Ambulatory Blood Pressure Monitoring in Sub-Saharan Africa: Hypertension Phenotypes and Dipping Patterns in Malawian HIV+ Patients on Antiretroviral Therapy
Abstract
Background: Cardiovascular disease and especially hypertension are a growing problem among people living with HIV (PLHIV) on antiretroviral therapy (ART) in sub-Saharan Africa.
Objectives: As robust data on hypertension phenotypes associated with distinct cardiovascular risks among PLHIV are limited, we aimed to assess the frequency of white-coat (WCH), masked (MH) hypertension, and blood pressure dipping-patterns in a group of Malawian PLHIV.
Methods: As part of the prospective Lighthouse-Tenofovir-Cohort-Study, we analyzed clinical, laboratory and 24-h-ambulatory blood pressure monitoring (ABPM) data of PLHIV from urban Lilongwe with treated or untreated hypertension or raised office blood pressure (OBP) during routine study-visits.
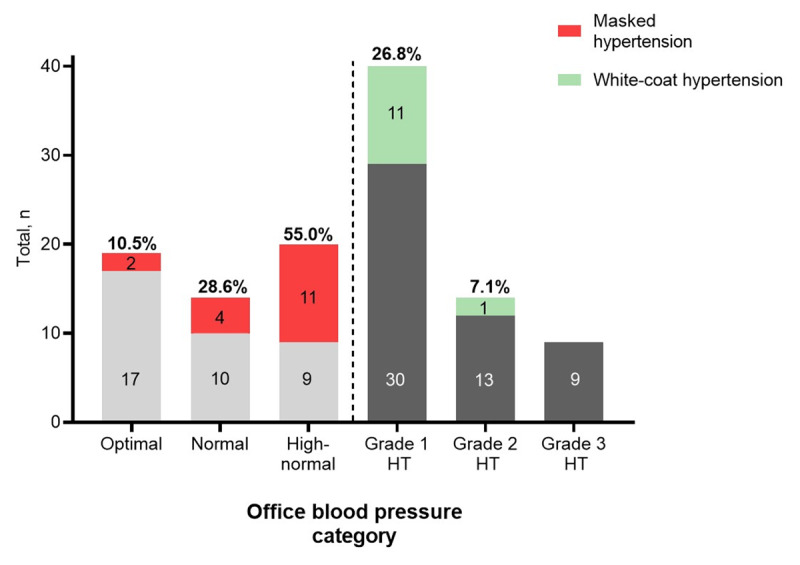
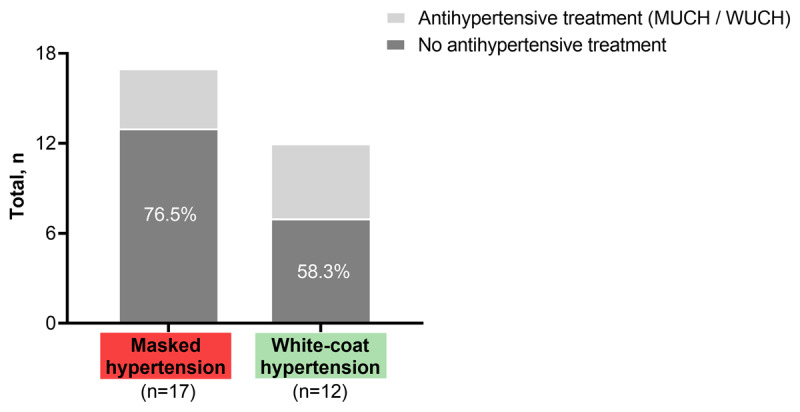
Results: 118 PLHIV were included and data of 117 participants could be analyzed. Twenty-four-hour ABPM normotension was found in a total of 73 PLHIV including 14/37 on antihypertensive treatment (37.8%). Using strict definitions, i.e. normal OBP plus normal mean BP for all periods of ABPM, controlled hypertension was found in only 4/37 (10.8%) PLHIV on antihypertensive treatment while true normotension was observed in 10/24 untreated patients (41.7%) with previously diagnosed hypertension and 22/56 patients (39.3%) without a medical history of hypertension. WCH with normal BP during all periods of 24-h-ABPM was identified in 12/64 OBP-hypertensive PLHIV (18.8%), primarily in patients with grade 1 hypertension (11/41 patients; 26.8%). MH was found in 17/53 PLHIV with OBP-normotension (32.1%), predominantly in patients with high normal BP (11/20 patients; 55%). The estimated glomerular filtration rate tended to be lower in MH compared to strictly defined normotensive PLHIV (92.0±20.4 vs. 104.8±15.7 ml/min/m²). 64.1 percent of PLHIV (59.5% with 24-h hypertension and 66.7% with 24-h normotension) had abnormal systolic dipping.
Conclusion: The high prevalence of WCH and MH with signs of early renal end-organ damage and an abnormal dipping in approximately 2/3 of PLHIV warrants further investigation as these factors may contribute to the increased cardiovascular risk in PLHIV in resource-limited settings like Malawi.
Clinical trial registration: https://clinicaltrials.gov (NCT02381275), registered March 6th, 2015.
Keywords: 24-hour ambulatory blood pressure monitoring; HIV; abnormal blood pressure dipping; masked hypertension; sub-Saharan Africa; white-coat hypertension.
Copyright: © 2021 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Blood pressure changes during tenofovir-based antiretroviral therapy among people living with HIV in Lilongwe, Malawi: results from the prospective LighTen Cohort Study.Clin Res Cardiol. 2023 Nov;112(11):1650-1663. doi: 10.1007/s00392-023-02253-w. Epub 2023 Jul 6. Clin Res Cardiol. 2023. PMID: 37414923 Free PMC article.
-
Office blood pressure versus ambulatory blood pressure measurement in childhood obesity.BMC Pediatr. 2023 Apr 29;23(1):205. doi: 10.1186/s12887-023-04010-4. BMC Pediatr. 2023. PMID: 37120521 Free PMC article.
-
Target organ damage in "white coat hypertension" and "masked hypertension".Am J Hypertens. 2008 Apr;21(4):393-9. doi: 10.1038/ajh.2008.15. Epub 2008 Feb 21. Am J Hypertens. 2008. PMID: 18292757
-
Mechanisms Influencing Circadian Blood Pressure Patterns Among Individuals with HIV.Curr Hypertens Rep. 2015 Nov;17(11):88. doi: 10.1007/s11906-015-0598-1. Curr Hypertens Rep. 2015. PMID: 26429228 Review.
-
Task force IV: Clinical use of ambulatory blood pressure monitoring. Participants of the 1999 Consensus Conference on Ambulatory Blood Pressure Monitoring.Blood Press Monit. 1999 Dec;4(6):319-31. doi: 10.1097/00126097-199912000-00005. Blood Press Monit. 1999. PMID: 10602536 Review.
Cited by
-
Hypertension among people living with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis.Sci Rep. 2024 Jul 23;14(1):16858. doi: 10.1038/s41598-024-67703-5. Sci Rep. 2024. PMID: 39039244 Free PMC article.
-
Blood pressure changes during tenofovir-based antiretroviral therapy among people living with HIV in Lilongwe, Malawi: results from the prospective LighTen Cohort Study.Clin Res Cardiol. 2023 Nov;112(11):1650-1663. doi: 10.1007/s00392-023-02253-w. Epub 2023 Jul 6. Clin Res Cardiol. 2023. PMID: 37414923 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
