

Association of Hypertension and Diabetes with Ischemic Heart Disease and Stroke Mortality in India: The Million Death Study
- PMID: 34692394
- PMCID: PMC8516008
- DOI: 10.5334/gh.1048
Association of Hypertension and Diabetes with Ischemic Heart Disease and Stroke Mortality in India: The Million Death Study
Abstract
Background: The cardiovascular outcomes of hypertension and diabetes in India have never been studied at the national level.
Objectives: We conducted a nationally-representative proportional mortality study to measure the associations of hypertension and diabetes with premature mortality due to ischemic heart disease (IHD) and stroke among Indian adults.
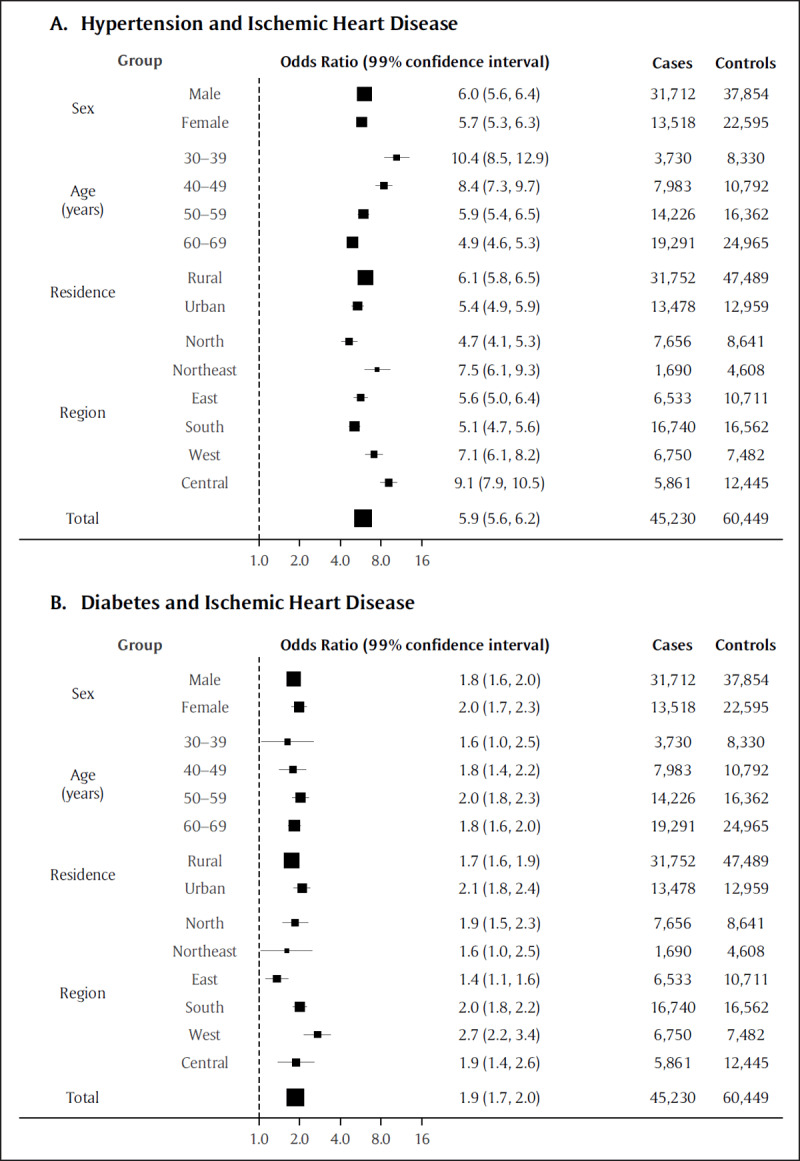
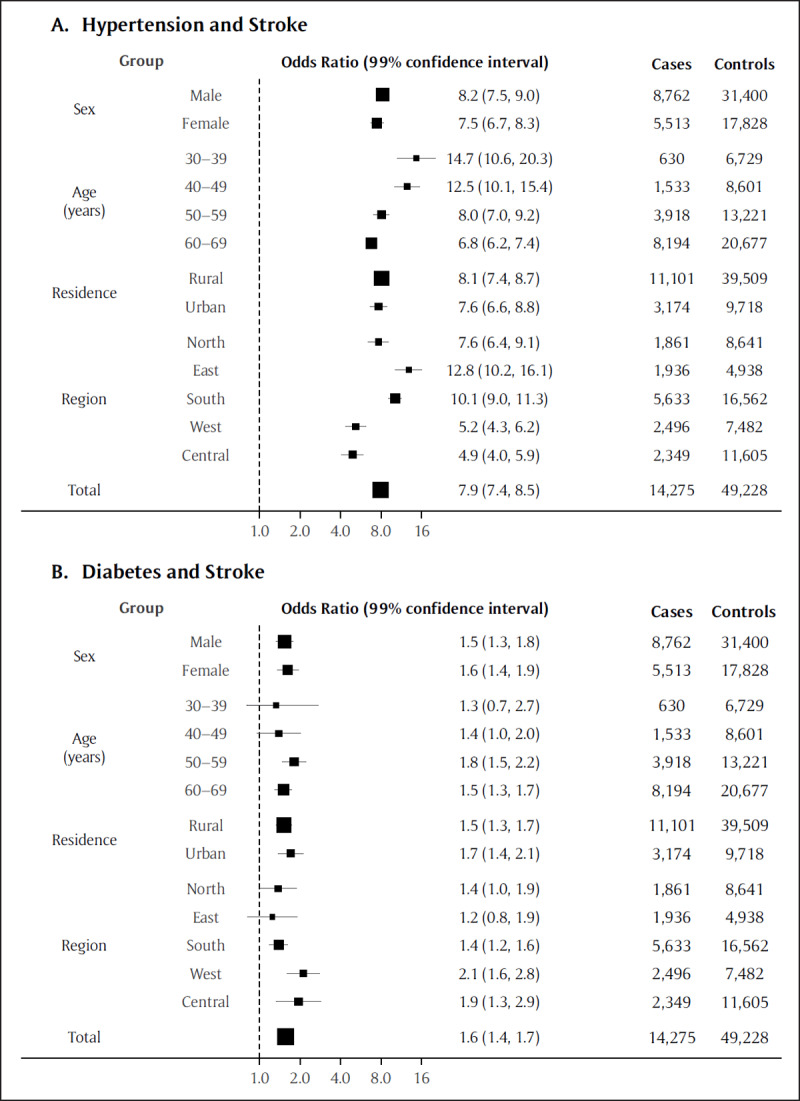
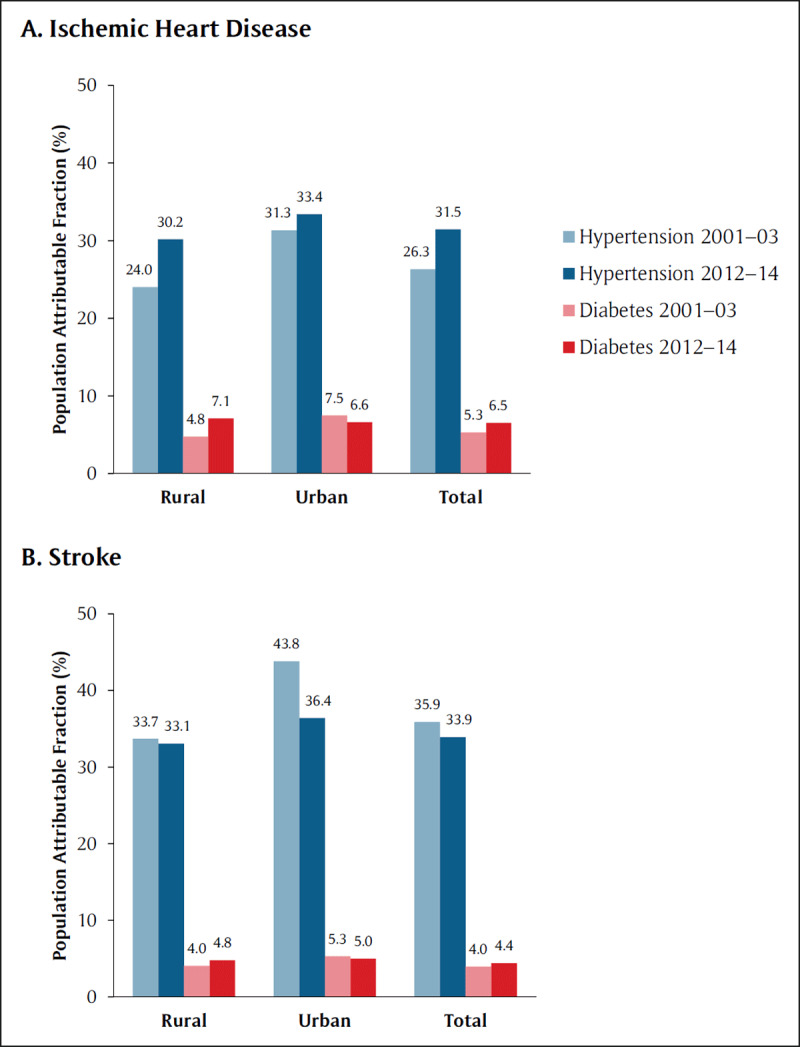
Methods: We determined causes of death by verbal autopsy from 2001-14 among 2.4 million households. We defined cases as those who died of the study outcomes and controls as those who died of injuries, respiratory causes, or cancer. We used multivariable logistic regression models to compute adjusted odds ratios (OR) measuring the association of hypertension and diabetes with IHD or stroke mortality, population-attributable fractions (PAF), and time trends.
Results: The mean age at death was 55.6 (standard deviation 9.9) years for IHD, 58.2 (9.0) years for stroke, and 46.8 (injury) to 59.8 (respiratory) years for controls. There were more men among both the cases (IHD: 70.1%; stroke: 59.0%) and controls (injury: 76.6%; cancer: 55.4%; respiratory: 59.8%). Hypertension was associated with six- to eight-fold increases in the odds of IHD (OR 5.9, 99% CI 5.6-6.2) and stroke mortality (7.9, 7.4-8.5). Diabetes was associated with double the odds (1.9, 1.7-2.0) of IHD mortality and increased odds of stroke mortality (1.6, 1.4-1.7). Hypertension accounted for an increasing PAF of IHD mortality and decreasing PAF of stroke mortality. Diabetes was associated with relatively lower PAFs and variable time trends.
Conclusions: Hypertension is associated with an unexpectedly high burden of cardiovascular mortality, and contributes to an increasing proportion of IHD deaths and a decreasing proportion of stroke deaths. Better management of hypertension and diabetes is urgently required to reduce premature cardiovascular mortality.
Keywords: cardiovascular disease; epidemiology; mortality; nationally representative.
Copyright: © 2021 The Author(s).
Conflict of interest statement
DX reports grants from Cadila Pharmaceuticals, grants from Boehringer Ingelheim, grants from Sanofi Aventis, grants from Pfizer, grants from Bristol Myers Squibb, grants from United Health, outside the submitted work. The other authors have no conflicts of interest to disclose.
Figures
References
-
- World Health Organization. Global Health Estimates 2015: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2015 [Internet]. Geneva: World Health Organization; 2016. [cited 13 August 2021]. Retrieved from: http://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.....
-
- Yusuf S, Joseph P, Rangarajan S, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155,722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. The Lancet. 7 March 2020; 395(10226): 795–808. DOI: 10.1016/S0140-6736(19)32008-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
