

First Attempt at Using Electrical Impedance Tomography to Predict High Flow Nasal Cannula Therapy Outcomes at an Early Phase
- PMID: 34692729
- PMCID: PMC8533818
- DOI: 10.3389/fmed.2021.737810
First Attempt at Using Electrical Impedance Tomography to Predict High Flow Nasal Cannula Therapy Outcomes at an Early Phase
Abstract
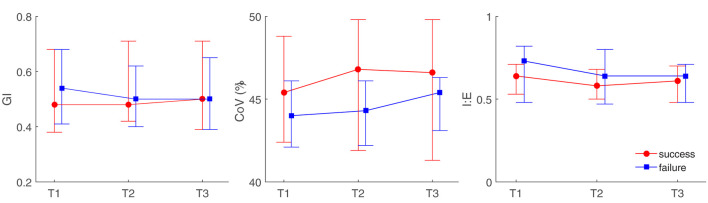
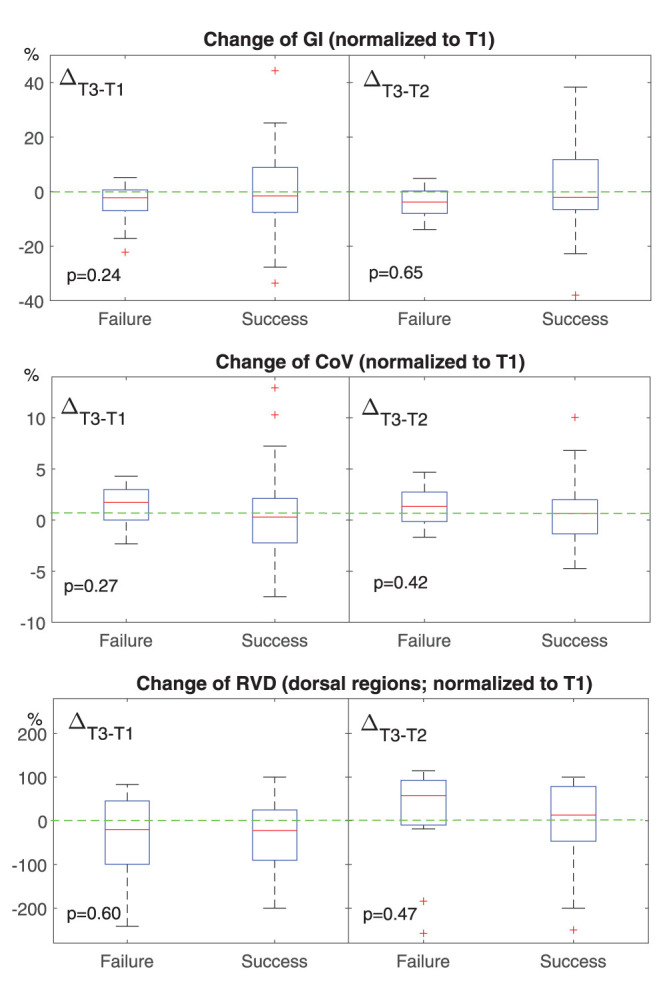
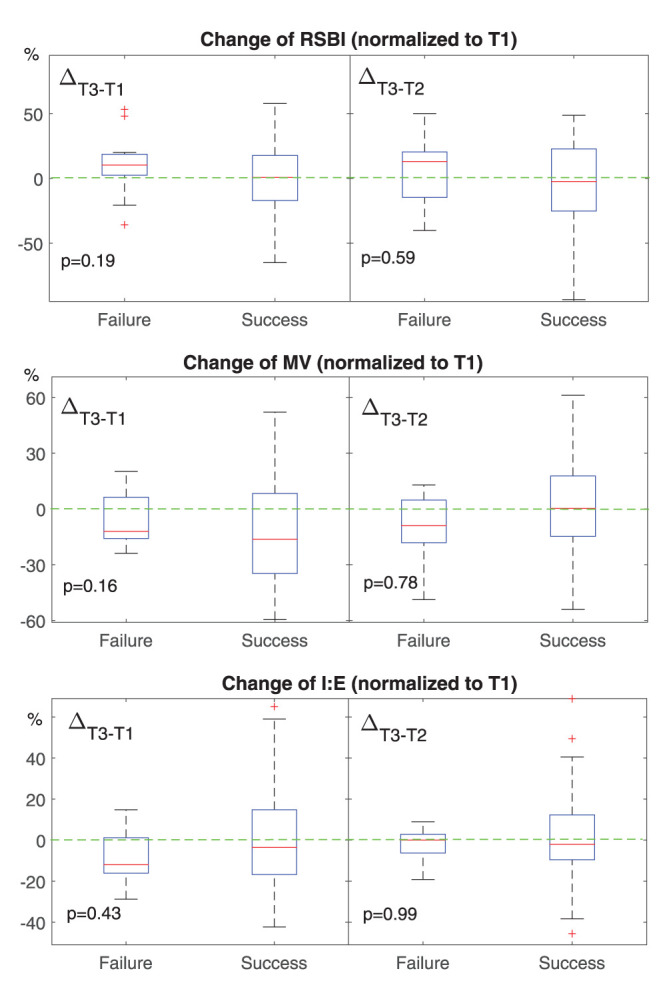
Objective: Spatial and temporal ventilation distributions in patients with acute respiratory failure during high flow nasal cannula (HFNC) therapy were previously studied with electrical impedance tomography (EIT). The aim of the study was to explore the possibility of predicting HFNC failure based on various EIT-derived parameters. Methods: High flow nasal cannula failure was defined reintubation within 48 h after HFNC. EIT was performed with the patients spontaneously breathing in the supine position at the start of HFNC. EIT-based indices (comprising the global inhomogeneity index, center of ventilation, ventilation delay, rapid shallow breathing index, minute volume, and inspiration to expiration time) were explored and evaluated at three time points (prior to HFNC, T1; 30 min after HFNC started, T2; and 1 h after, T3). Results: A total of 46 subjects were included in the final analysis. Eleven subjects had failed HFNC. The time to failure was 27.8 ± 12.4 h. The ROX index (defined as SpO2/FiO2/respiratory rate) for HFNC success patients was 8.3 ± 2.7 and for HFNC failure patients, 6.2 ± 1.8 (p = 0.23). None of the investigated EIT-based parameters showed significant differences between subjects with HFNC failure and success. Further subgroup analysis indicated that a significant difference in ventilation inhomogeneity was found between ARDS and non-ARDS [0.54 (0.37) vs. 0.46 (0.28) as evaluated with GI, p < 0.01]. Ventilation homogeneity significantly improved in ARDS after 60-min HFNC treatment [0.59 (0.20) vs 0.57 (0.19), T1 vs. T3, p < 0.05]. Conclusion: Spatial and temporal ventilation distributions were slightly but insignificantly different between the HFNC success and failure groups. HFNC failure could not be predicted by changes in EIT temporal and spatial indexes of ventilation distribution within the first hour. Further studies are required to predict the outcomes of HFNC.
Keywords: acute respiratory failure; electrical impedance tomography; high flow nasal cannula; outcome prediction; ventilation distribution.
Copyright © 2021 Li, Zhang, Xia, Xu, Qin, Dai, Fu, Gao and Zhao.
Conflict of interest statement
ZZhao receives a consulting fee from Drager Medical. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Investigation of high flow nasal cannule efficiency with electric impedance tomography based parameters in COVID-19 adults patients: a retrospective study.PeerJ. 2023 Jul 14;11:e15555. doi: 10.7717/peerj.15555. eCollection 2023. PeerJ. 2023. PMID: 37465153 Free PMC article.
-
Effects of High-Flow Nasal Cannula on End-Expiratory Lung Impedance in Semi-Seated Healthy Subjects.Respir Care. 2018 Aug;63(8):1016-1023. doi: 10.4187/respcare.06031. Epub 2018 Jun 26. Respir Care. 2018. PMID: 29945910
-
Effect of postextubation high-flow nasal cannula therapy on lung recruitment and overdistension in high-risk patient.Crit Care. 2020 Mar 6;24(1):82. doi: 10.1186/s13054-020-2809-7. Crit Care. 2020. PMID: 32143664 Free PMC article.
-
Performance of the ROX index in predicting high flow nasal cannula failure in COVID-19 patients: a systematic review and meta-analysis.Crit Care. 2023 Aug 21;27(1):320. doi: 10.1186/s13054-023-04567-7. Crit Care. 2023. PMID: 37605238 Free PMC article.
-
The ROX index as a predictor of high-flow nasal cannula outcome in pneumonia patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis.BMC Pulm Med. 2022 Apr 1;22(1):121. doi: 10.1186/s12890-022-01914-2. BMC Pulm Med. 2022. PMID: 35365110 Free PMC article.
Cited by
-
Prediction of high-flow nasal cannula outcomes at the early phase using the modified respiratory rate oxygenation index.BMC Pulm Med. 2022 Jun 13;22(1):227. doi: 10.1186/s12890-022-02017-8. BMC Pulm Med. 2022. PMID: 35698120 Free PMC article.
-
Volume-OXygenation Index to Predict High-flow Nasal Cannula Failure: How to Capture the Tidal Volume Matters.Am J Respir Crit Care Med. 2023 Feb 15;207(4):490-491. doi: 10.1164/rccm.202209-1659LE. Am J Respir Crit Care Med. 2023. PMID: 36198170 Free PMC article. No abstract available.
-
Monitoring the Efficacy of High-Flow Nasal Cannula Oxygen Therapy in Patients with Acute Hypoxemic Respiratory Failure in the General Respiratory Ward: A Prospective Observational Study.Biomedicines. 2023 Nov 16;11(11):3067. doi: 10.3390/biomedicines11113067. Biomedicines. 2023. PMID: 38002067 Free PMC article.
-
Investigation of high flow nasal cannule efficiency with electric impedance tomography based parameters in COVID-19 adults patients: a retrospective study.PeerJ. 2023 Jul 14;11:e15555. doi: 10.7717/peerj.15555. eCollection 2023. PeerJ. 2023. PMID: 37465153 Free PMC article.
-
Bedside electrical impedance tomography to assist the management of pulmonary embolism: A case report.Heliyon. 2024 Jan 26;10(3):e25159. doi: 10.1016/j.heliyon.2024.e25159. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38322858 Free PMC article.
References
LinkOut - more resources
Full Text Sources