

Tuberculosis endotypes to guide stratified host-directed therapy
- PMID: 34693385
- PMCID: PMC8530349
- DOI: 10.1016/j.medj.2020.11.003
Tuberculosis endotypes to guide stratified host-directed therapy
Abstract
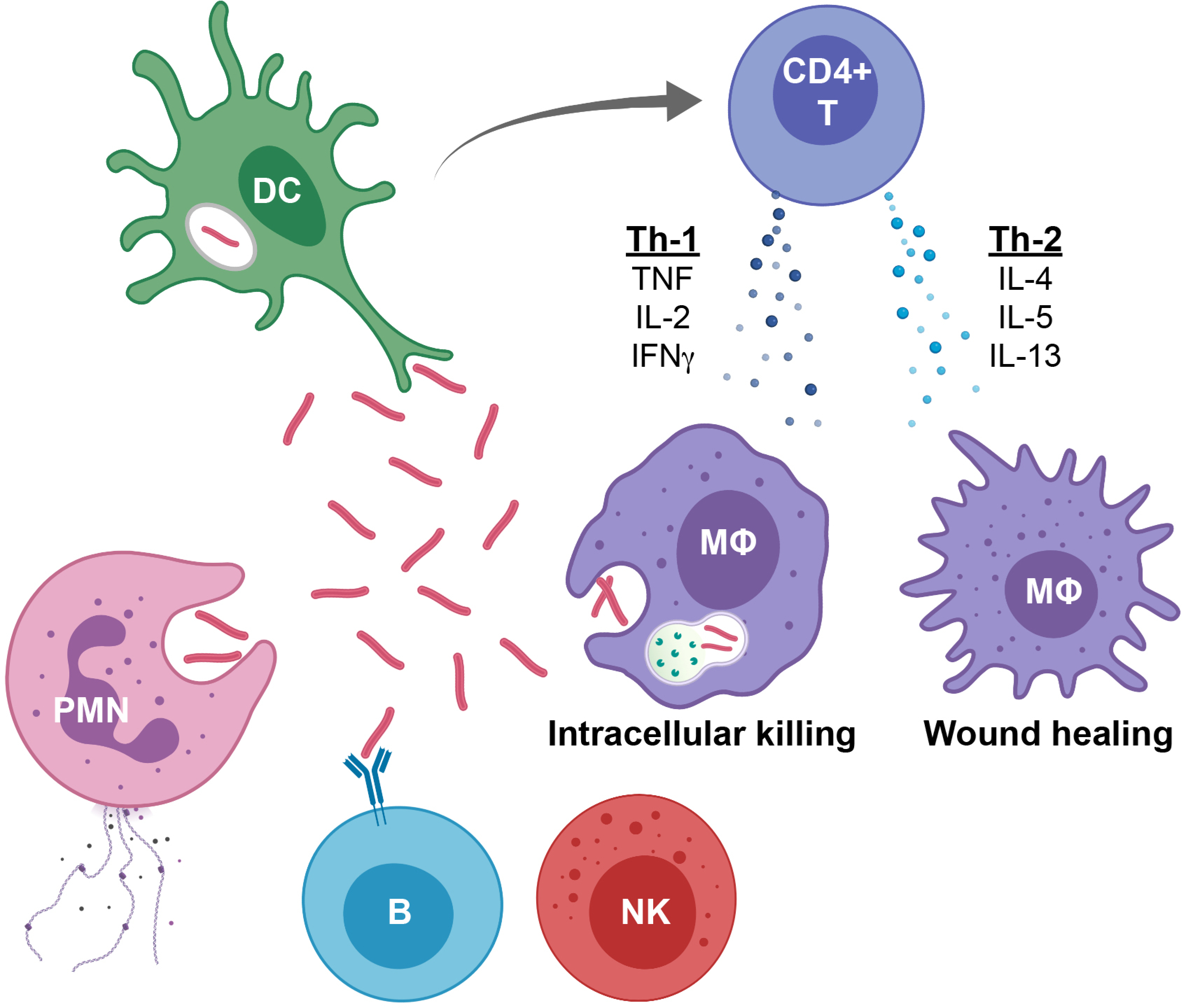
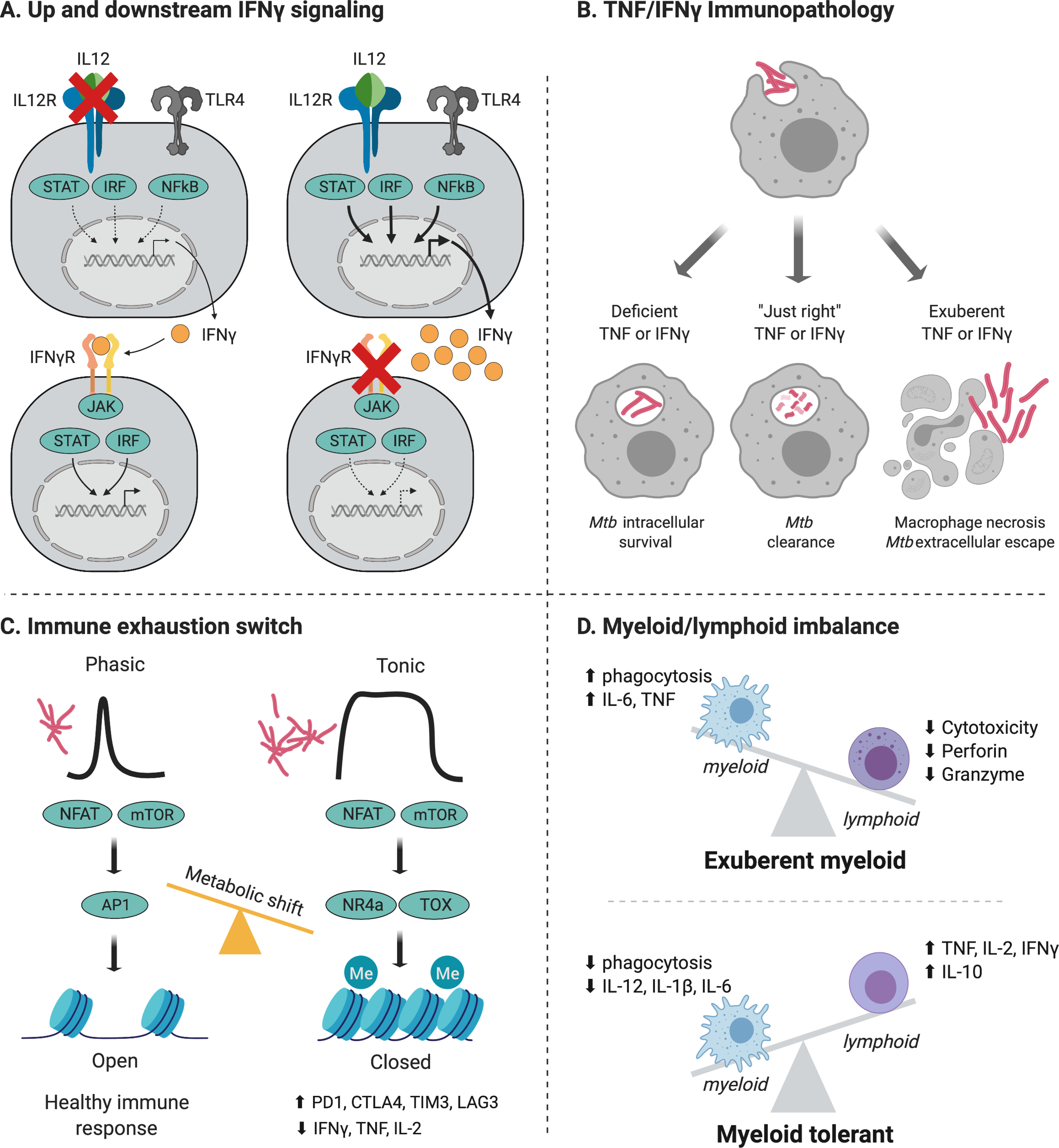
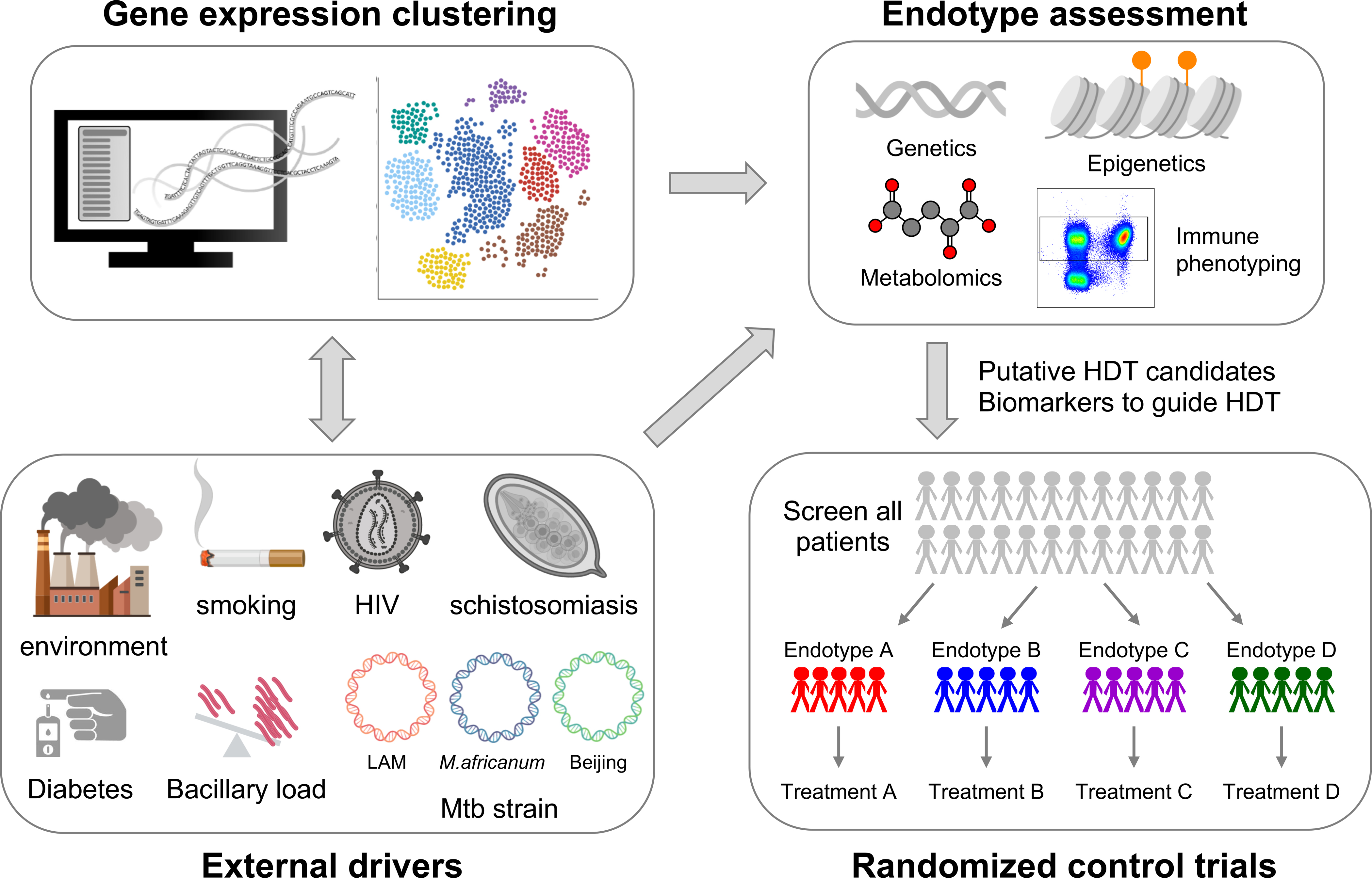
There is hope that host-directed therapy (HDT) for Tuberculosis (TB) can either shorten treatment duration, help cure drug resistant disease or limit the immunopathology. Many candidate HDT drugs have been proposed, however solid evidence only exists for a few select patient groups. The clinical presentation of TB is variable, with differences in severity, tissue pathology, and bacillary burden. TB clinical phenotypes likely determine the potential benefit of HDT. Underlying TB clinical phenotypes, there are TB "endotypes," defined as distinct molecular profiles, with specific metabolic, epigenetic, transcriptional, and immune phenotypes. TB endotypes can be characterized by either immunodeficiency or pathologic excessive inflammation. Additional factors, like comorbidities (HIV, diabetes, helminth infection), structural lung disease or Mycobacterial virulence also drive TB endotypes. Precise disease phenotyping, combined with in-depth immunologic and molecular profiling and multimodal omics integration, can identify TB endotypes, guide endotype-specific HDT, and improve TB outcomes, similar to advances in cancer medicine.
Keywords: Tuberculosis; endotypes; immune correlates of protection.
Figures
References
-
- Meintjes G, Stek C, Blumenthal L, Thienemann F, Schutz C, Buyze J, et al. Prednisone for the Prevention of Paradoxical Tuberculosis-Associated IRIS. The New England journal of medicine. 2018;379(20):1915–25. - PubMed
-
- Lotvall J, Akdis CA, Bacharier LB, Bjermer L, Casale TB, Custovic A, et al. Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. The Journal of allergy and clinical immunology. 2011;127(2):355–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical