

Mechanisms and management of prothrombotic state in COVID-19 disease
- PMID: 34693818
- PMCID: PMC8785300
- DOI: 10.1177/17539447211053470
Mechanisms and management of prothrombotic state in COVID-19 disease
Abstract
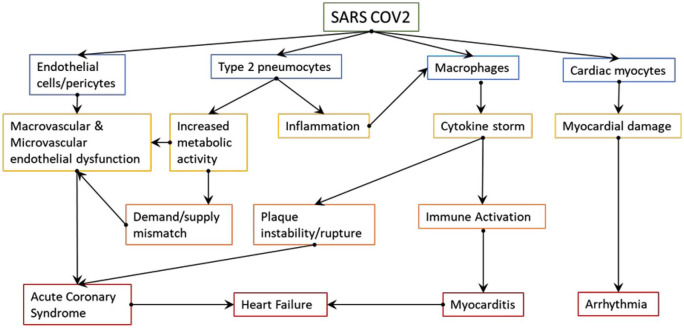
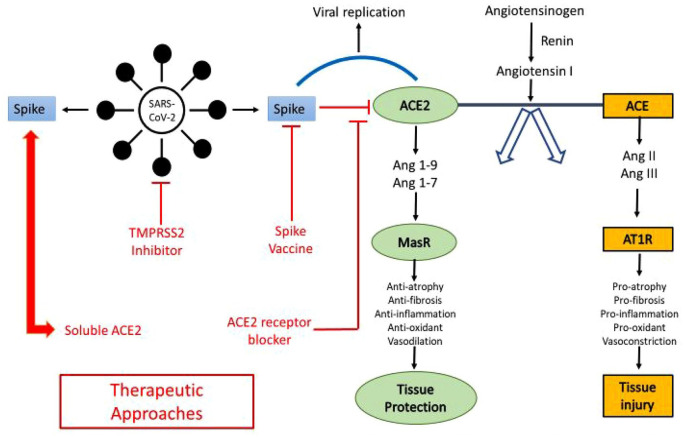
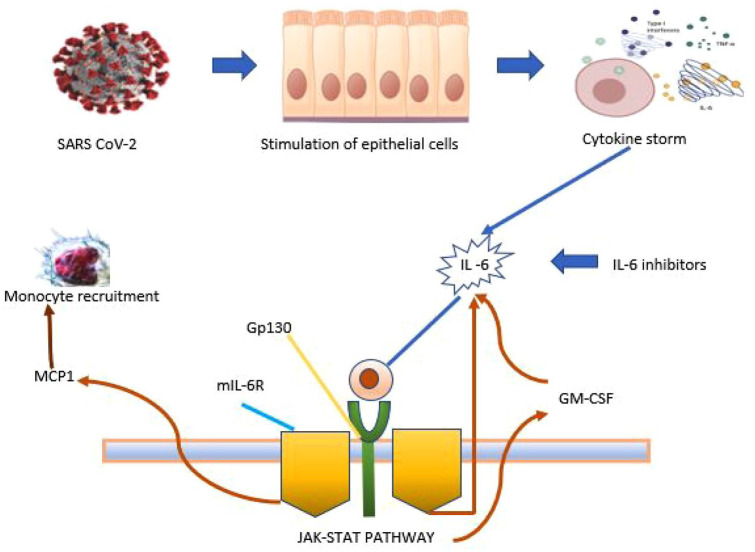
The novel severe acute respiratory syndrome viral disease outbreak due to SARS-CoV-2 is a rapidly evolving disease and represents one of the greatest medical challenges in recent times. It is believed that SARS-CoV-2 has migrated from bats to an intermediate host and then to humans. This article aims at the mechanism and management of prothrombotic state in COVID-19 positive patients. We tried to present how the SARS-CoV-2 virus can induce thromboembolic events and the incidence of these thromboembolic events. We also tried to depict anticoagulation management in these patients as well as postdischarge plan and follow-up. Invasion of type 2 pneumocytes by the SARS-CoV-2 virus is critical in the course of illness because it results in activation of immune cells leading to elevation of cytokines. The subsequent activation of T cells and macrophages infiltrates the infected myocardial cells causing direct myocardiocyte toxicity and development of arrhythmia. Hypoxia or hypotension during the clinical course causes a mismatch between myocyte oxygen supply and workload demand resulting in cardiac distress. SARS-CoV-2 affects endothelial cells and pericytes that lead to severe micro and macrovascular dysfunction, and together with oxygen supply-demand mismatch, immune hyperresponsivity can potentially cause destabilization and plaque rupture causing acute coronary syndromes. Other mechanisms of injury include myocarditis, pericarditis, stress cardiomyopathy, vasculitis, and DIC (Disseminated intravascular coagulation)/microthrombi. SARS-CoV-2 enters the cells by the Spike protein S whose surface unit, S1, binds to the ACE2 receptor on the host cell. The type II transmembrane serine proteases TMPRSS2 and histone acetyltransferases (HAT) are host cell proteases that are recruited by the virus to cleave ACE2 surface protein S which facilitates the viral entry. Therefore, TMPRSS2 and HAT could be targeted for potential drugs against SARS-CoV-2. SARS-CoV-2 uses an RNA-dependent RNA polymerase for proliferation, which is targeted by remdesivir that is currently approved for emergency use by Food and Drug Administration (FDA). We need to adopt a multifaceted approach when combating SARS-CoV-2 because it presents several challenges including medical, psychological, socioeconomic, and ethical. COVID-19 is the biggest calamity during the 21st century, we need to have a keen understanding of its pathophysiology and clinical implications for the development of preventive measures and therapeutic modalities.
Keywords: COVID-19; anticoagulation of choice; cardiovascular complications; prothrombotic state.
Conflict of interest statement
Figures
Similar articles
-
SARS-CoV-2 strategically mimics proteolytic activation of human ENaC.Elife. 2020 May 26;9:e58603. doi: 10.7554/eLife.58603. Elife. 2020. PMID: 32452762 Free PMC article.
-
Single-cell analysis of SARS-CoV-2 receptor ACE2 and spike protein priming expression of proteases in the human heart.Cardiovasc Res. 2020 Aug 1;116(10):1733-1741. doi: 10.1093/cvr/cvaa191. Cardiovasc Res. 2020. PMID: 32638018 Free PMC article.
-
ZMPSTE24 Regulates SARS-CoV-2 Spike Protein-enhanced Expression of Endothelial PAI-1.Am J Respir Cell Mol Biol. 2021 Sep;65(3):300-308. doi: 10.1165/rcmb.2020-0544OC. Am J Respir Cell Mol Biol. 2021. PMID: 34003736 Free PMC article.
-
Pathogenesis-directed therapy of 2019 novel coronavirus disease.J Med Virol. 2021 Mar;93(3):1320-1342. doi: 10.1002/jmv.26610. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33073355 Review.
-
Cell-Specific Mechanisms in the Heart of COVID-19 Patients.Circ Res. 2023 May 12;132(10):1290-1301. doi: 10.1161/CIRCRESAHA.123.321876. Epub 2023 May 11. Circ Res. 2023. PMID: 37167361 Free PMC article. Review.
Cited by
-
Pathophysiological Mechanisms Linking COVID-19 and Acute Surgical Abdomen: A Literature Review.Life (Basel). 2025 Apr 27;15(5):707. doi: 10.3390/life15050707. Life (Basel). 2025. PMID: 40430138 Free PMC article. Review.
-
COVID-19 complicating pregnancy: A retrospective study of nine intensive care unit patients.Obstet Med. 2024 Mar;17(1):28-35. doi: 10.1177/1753495X231169849. Epub 2023 May 8. Obstet Med. 2024. PMID: 38655195 Free PMC article.
-
Low dose ultra-slow infusion thrombolytic therapy (LDUSITT) as an alternative option in a COVID-19 patient with free-floating right atrial thrombus: a case report and review of literature.Thromb J. 2023 Jan 30;21(1):12. doi: 10.1186/s12959-023-00457-8. Thromb J. 2023. PMID: 36710332 Free PMC article.
-
Anticoagulation strategies in COVID-19 infected patients receiving ECMO support.J Extra Corpor Technol. 2023 Sep;55(3):121-129. doi: 10.1051/ject/2023027. Epub 2023 Sep 8. J Extra Corpor Technol. 2023. PMID: 37682210 Free PMC article.
-
A Perfect Storm: Ventricular Fibrillation Cardiac Arrest Due to Acute Myocardial Infarction Seen in the Postpartum Period in the Setting of COVID.Cureus. 2023 Jun 22;15(6):e40782. doi: 10.7759/cureus.40782. eCollection 2023 Jun. Cureus. 2023. PMID: 37485131 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
