

Noninvasive respiratory support for acute respiratory failure due to COVID-19
- PMID: 34694240
- PMCID: PMC8711305
- DOI: 10.1097/MCC.0000000000000902
Noninvasive respiratory support for acute respiratory failure due to COVID-19
Abstract
Purpose of review: Noninvasive respiratory support has been widely applied during the COVID-19 pandemic. We provide a narrative review on the benefits and possible harms of noninvasive respiratory support for COVID-19 respiratory failure.
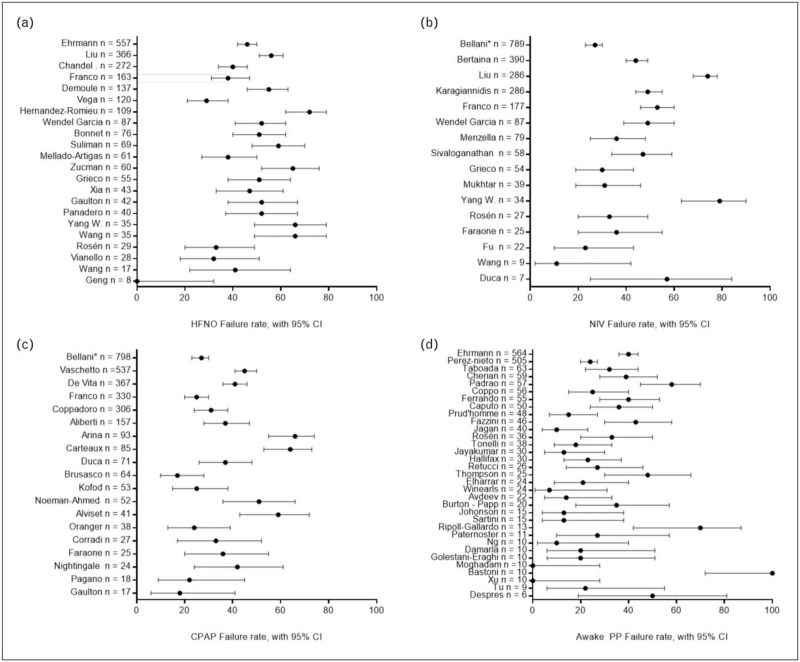
Recent findings: Maintenance of spontaneous breathing by means of noninvasive respiratory support in hypoxemic patients with vigorous spontaneous effort carries the risk of patient self-induced lung injury: the benefit of averting intubation in successful patients should be balanced with the harms of a worse outcome in patients who are intubated after failing a trial of noninvasive support.The risk of noninvasive treatment failure is greater in patients with the most severe oxygenation impairment (PaO2/FiO2 < 200 mmHg).High-flow nasal oxygen (HFNO) is the most widely applied intervention in COVID-19 patients with hypoxemic respiratory failure. Also, noninvasive ventilation (NIV) and continuous positive airway pressure delivered with different interfaces have been used with variable success rates. A single randomized trial showed lower need for intubation in patients receiving helmet NIV with specific settings, compared to HFNO alone.Prone positioning is recommended for moderate-to-severe acute respiratory distress syndrome patients on invasive ventilation. Awake prone position has been frequently applied in COVID-19 patients: one randomized trial showed improved oxygenation and lower intubation rate in patients receiving 6-h sessions of awake prone positioning, as compared to conventional management.
Summary: Noninvasive respiratory support and awake prone position are tools possibly capable of averting endotracheal intubation in COVID-19 patients; carefully monitoring during any treatment is warranted to avoid delays in endotracheal intubation, especially in patients with PaO2/FiO2 < 200 mmHg.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- World Heal Organ, WHO Headquarters. Clinical management Clinical management Living guidance COVID-19. 2021; https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1
-
- Rochwerg B, Brochard L, Elliott MW, et al. . Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J 2017; 50:1602426.doi: 10.1183/13993003.02426-2016. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
