

Assessment of Nonfatal Myocardial Infarction as a Surrogate for All-Cause and Cardiovascular Mortality in Treatment or Prevention of Coronary Artery Disease: A Meta-analysis of Randomized Clinical Trials
- PMID: 34694318
- PMCID: PMC8546625
- DOI: 10.1001/jamainternmed.2021.5726
Assessment of Nonfatal Myocardial Infarction as a Surrogate for All-Cause and Cardiovascular Mortality in Treatment or Prevention of Coronary Artery Disease: A Meta-analysis of Randomized Clinical Trials
Abstract
Importance: Although nonfatal myocardial infarction (MI) is associated with an increased risk of mortality, evidence validating nonfatal MI as a surrogate end point for all-cause or cardiovascular (CV) mortality is lacking.
Objective: To examine whether nonfatal MI may be a surrogate for all-cause or CV mortality in patients with or at risk for coronary artery disease.
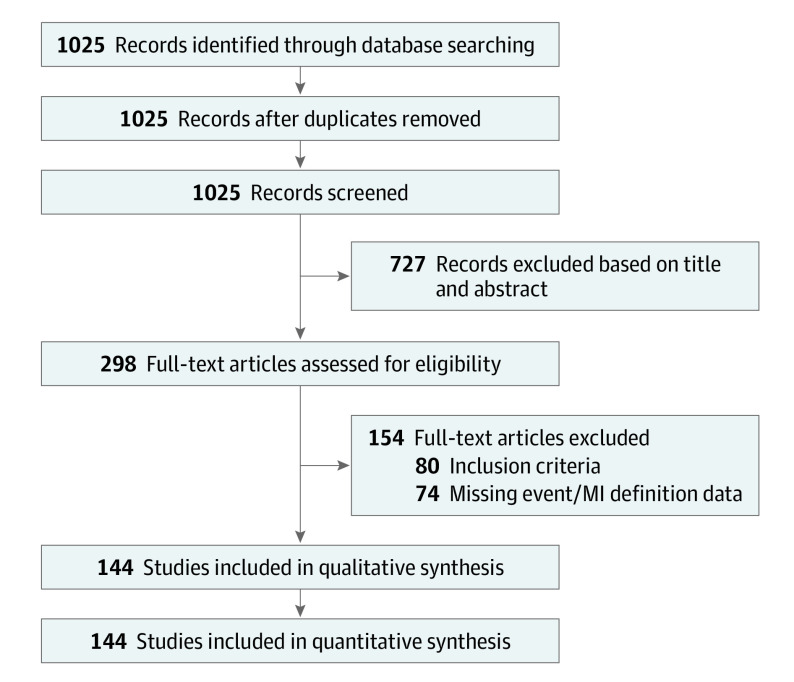
Data sources: In this meta-analysis, PubMed was searched from inception until December 31, 2020, for randomized clinical trials of interventions to treat or prevent coronary artery disease reporting mortality and nonfatal MI published in 3 leading journals.
Study selection: Randomized clinical trials including at least 1000 patients with 24 months of follow-up.
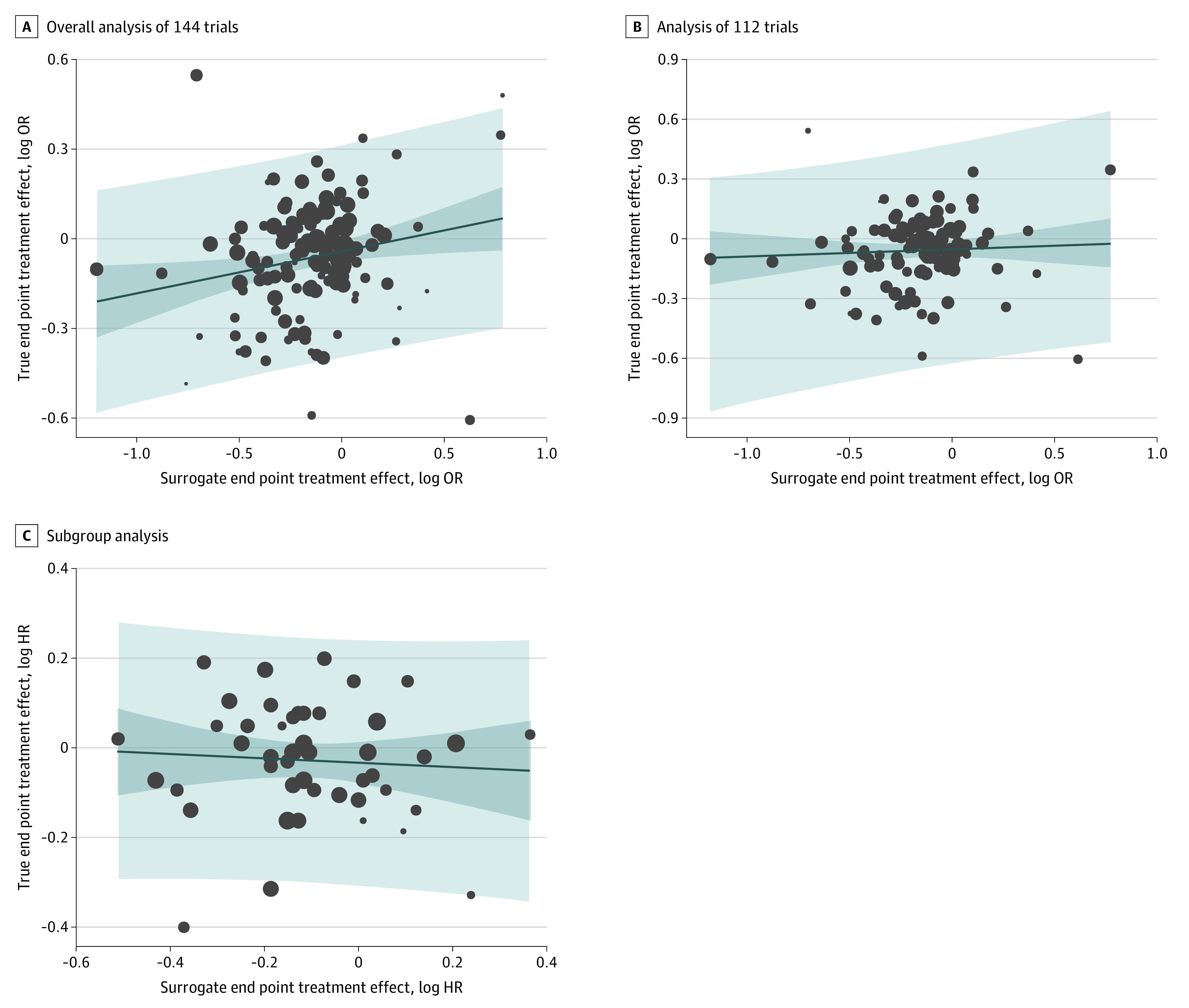
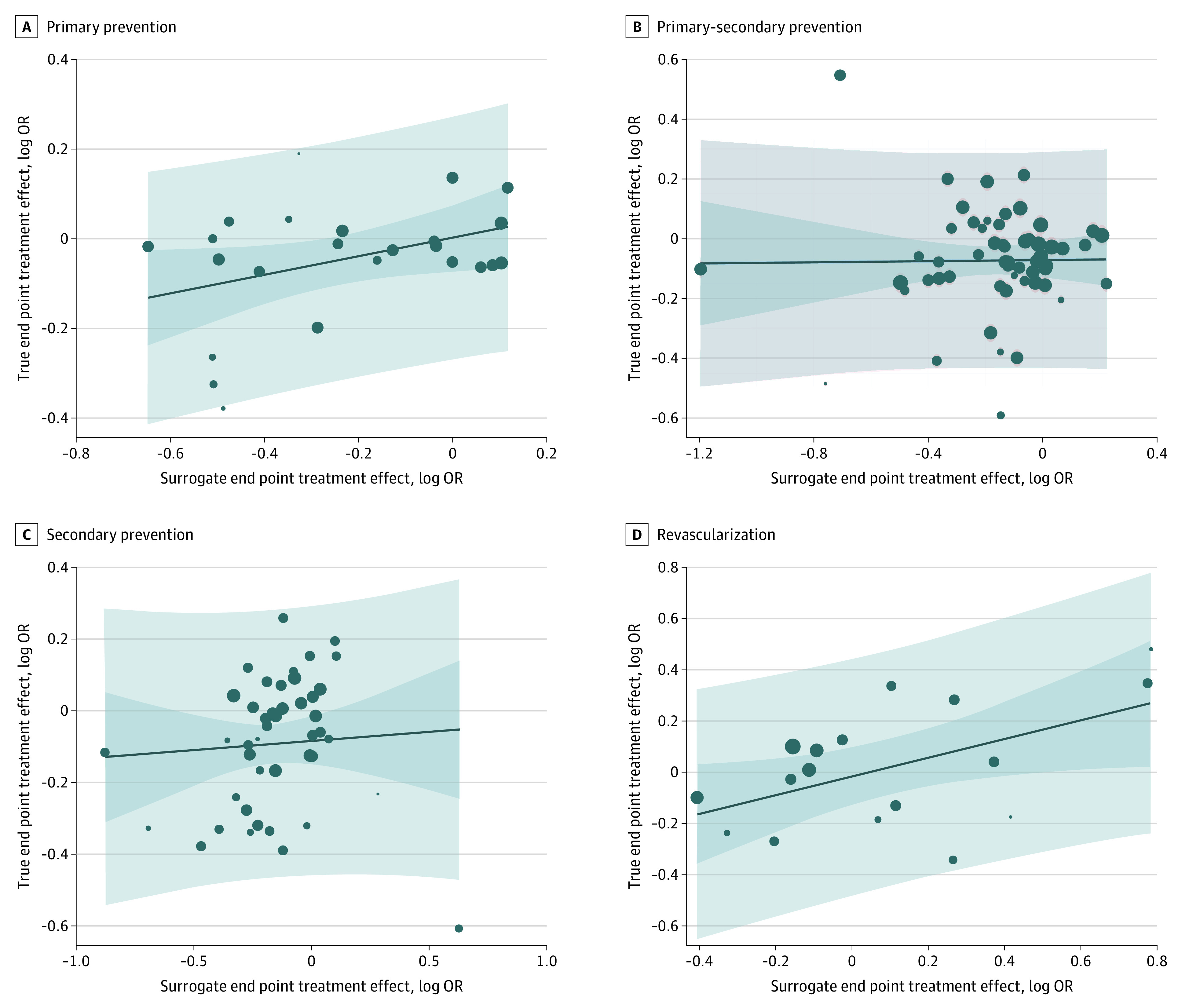
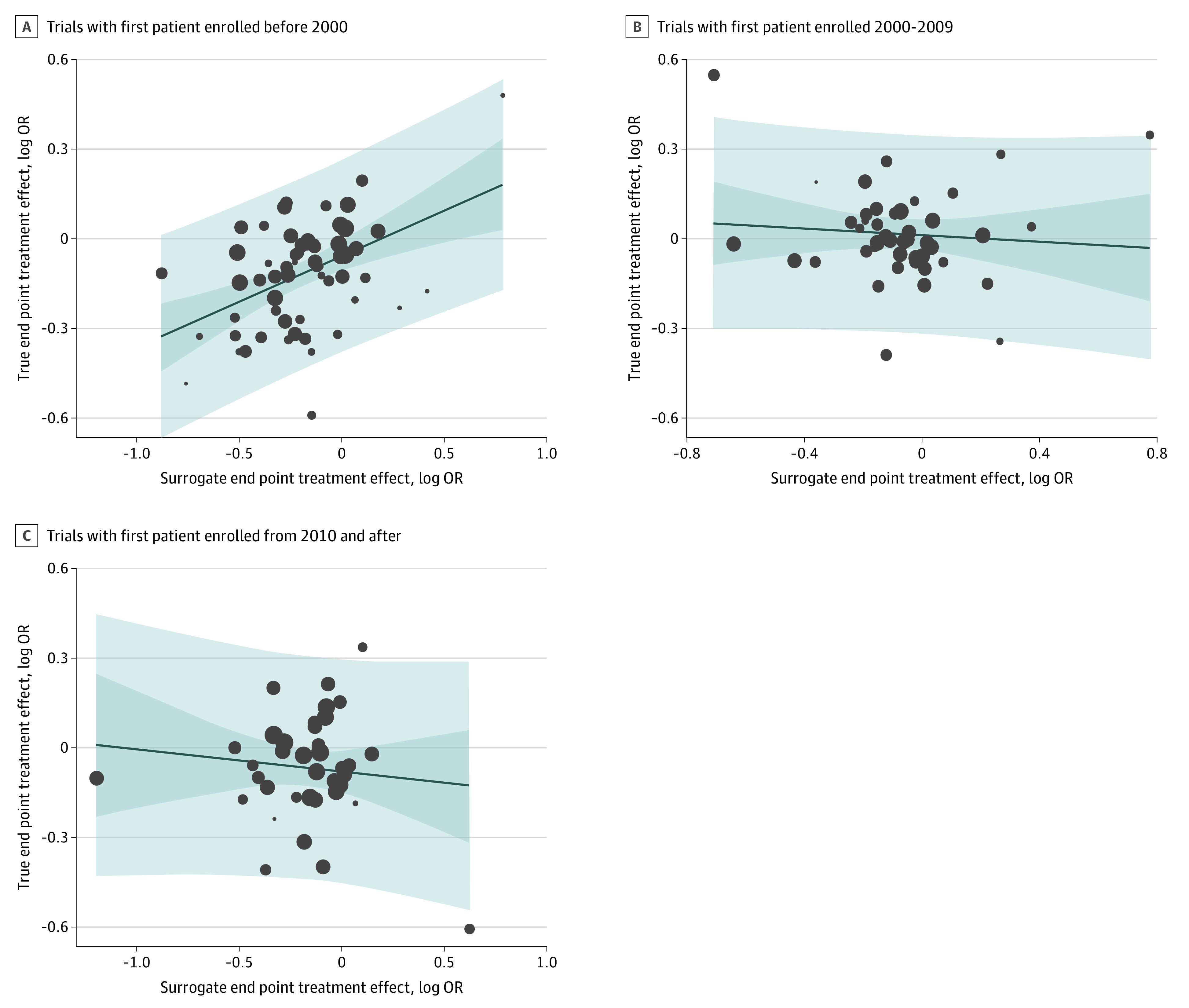
Data extraction and synthesis: Trial-level correlations between nonfatal MI and all-cause or CV mortality were assessed for surrogacy using the coefficient of determination (R2). The criterion for surrogacy was set at 0.8. Subgroup analyses based on study subject (primary prevention, secondary prevention, mixed primary and secondary prevention, and revascularization), era of trial (before 2000, 2000-2009, and 2010 and after), and follow-up duration (2.0-3.9, 4.0-5.9, and ≥6.0 years) were performed.
Main outcomes and measures: All-cause or CV mortality and nonfatal MI.
Results: A total of 144 articles randomizing 1 211 897 patients met the criteria for inclusion. Nonfatal MI did not meet the threshold for surrogacy for all-cause (R2 = 0.02; 95% CI, 0.00-0.08) or CV (R2 = 0.11; 95% CI, 0.02-0.27) mortality. Nonfatal MI was not a surrogate for all-cause mortality in primary (R2 = 0.01; 95% CI, 0.001-0.26), secondary (R2 = 0.03; 95% CI, 0.00-0.20), mixed primary and secondary prevention (R2 = 0.001; 95% CI, 0.00-0.08), or revascularization trials (R2 = 0.21; 95% CI, 0.002-0.50). For trials enrolling patients before 2000 (R2 = 0.22; 95% CI, 0.08-0.36), between 2000 and 2009 (R2 = 0.02; 95% CI, 0.00-0.17), and from 2010 and after (R2 = 0.01; 95% CI, 0.00-0.09), nonfatal MI was not a surrogate for all-cause mortality. Nonfatal MI was not a surrogate for all-cause mortality in randomized clinical trials with 2.0 to 3.9 (R2 = 0.004; 95% CI, 0.00-0.08), 4.0 to 5.9 (R2 = 0.06; 95% CI, 0.001-0.16), or 6.0 or more years of follow-up (R2 = 0.30; 95% CI, 0.01-0.55).
Conclusions and relevance: The findings of this meta-analysis do not appear to establish nonfatal MI as a surrogate for all-cause or CV mortality in randomized clinical trials of interventions to treat or prevent coronary artery disease.
Conflict of interest statement
Figures
Comment in
-
Nonfatal Myocardial Infarction-Poor Surrogate for Mortality.JAMA Intern Med. 2021 Dec 1;181(12):1588. doi: 10.1001/jamainternmed.2021.5713. JAMA Intern Med. 2021. PMID: 34694340 No abstract available.
-
Non-fatal MI as surrogate end point for all-cause or cardiovascular mortality.Nat Rev Cardiol. 2022 Mar;19(3):149-150. doi: 10.1038/s41569-021-00667-5. Nat Rev Cardiol. 2022. PMID: 35031686 No abstract available.
-
The Importance of Using the Appropriate Model for Systematic Reviews and Meta-analyses-Reply.JAMA Intern Med. 2022 Mar 1;182(3):357-358. doi: 10.1001/jamainternmed.2021.8132. JAMA Intern Med. 2022. PMID: 35099503 No abstract available.
-
The Importance of Using the Appropriate Model for Systematic Reviews and Meta-analyses.JAMA Intern Med. 2022 Mar 1;182(3):357. doi: 10.1001/jamainternmed.2021.8135. JAMA Intern Med. 2022. PMID: 35099524 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
