

Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 in Households with Children, Southwest Germany, May-August 2020
- PMID: 34695369
- PMCID: PMC8632156
- DOI: 10.3201/eid2712.210978
Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 in Households with Children, Southwest Germany, May-August 2020
Abstract
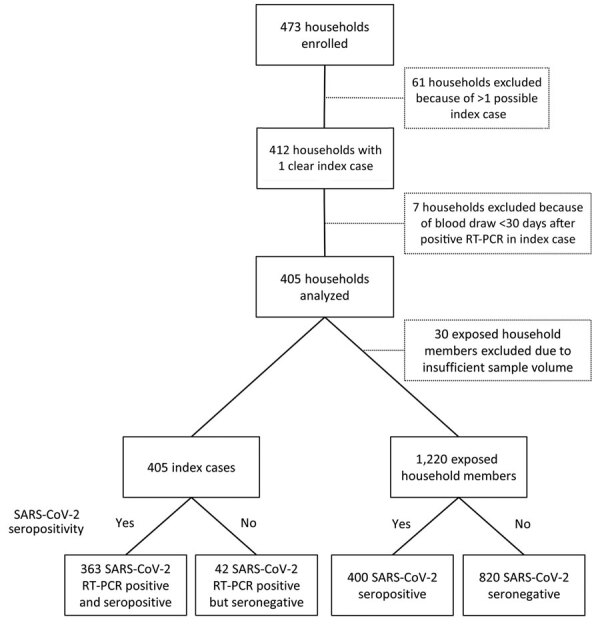
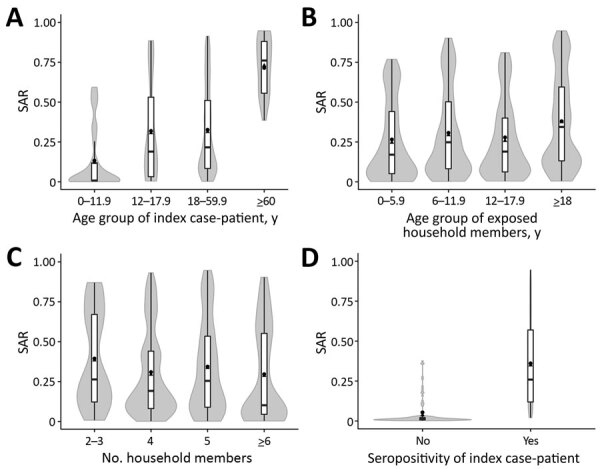
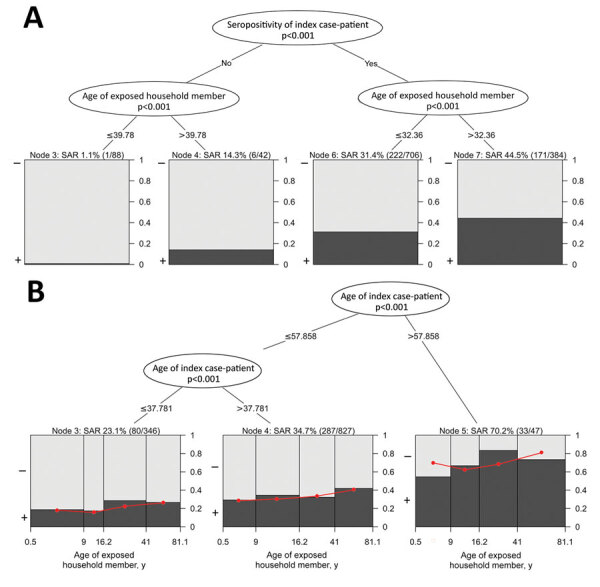
Resolving the role of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission in households with members from different generations is crucial for containing the current pandemic. We conducted a large-scale, multicenter, cross-sectional seroepidemiologic household transmission study in southwest Germany during May 11-August 1, 2020. We included 1,625 study participants from 405 households that each had ≥1 child and 1 reverse transcription PCR-confirmed SARS-CoV-2-infected index case-patient. The overall secondary attack rate was 31.6% and was significantly higher in exposed adults (37.5%) than in children (24.6%-29.2%; p = <0.015); the rate was also significantly higher when the index case-patient was >60 years of age (72.9%; p = 0.039). Other risk factors for infectiousness of the index case-patient were SARS-CoV-2-seropositivity (odds ratio [OR] 27.8, 95% CI 8.26-93.5), fever (OR 1.93, 95% CI 1.14-3.31), and cough (OR 2.07, 95% CI 1.21-3.53). Secondary infections in household contacts generate a substantial disease burden.
Keywords: COVID-19; SARS-CoV-2; antibodies; children; coronavirus disease; households; respiratory infections; serology; severe acute respiratory syndrome coronavirus 2; transmission; viruses; zoonoses.
Figures
Similar articles
-
Prevalence of SARS-CoV-2 Infection in Children and Their Parents in Southwest Germany.JAMA Pediatr. 2021 Jun 1;175(6):586-593. doi: 10.1001/jamapediatrics.2021.0001. JAMA Pediatr. 2021. PMID: 33480966 Free PMC article.
-
High prevalence of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) antibodies among unvaccinated children of Chandigarh, Northwest India, in a household-based paediatric serosurvey post-second wave of pandemic (June to July 2021).Public Health. 2023 Dec;225:160-167. doi: 10.1016/j.puhe.2023.10.010. Epub 2023 Nov 4. Public Health. 2023. PMID: 37931485
-
Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Dec 1;3(12):e2031756. doi: 10.1001/jamanetworkopen.2020.31756. JAMA Netw Open. 2020. PMID: 33315116 Free PMC article.
-
Incidence and Transmission of SARS-CoV-2 in US Child Care Centers After COVID-19 Vaccines.JAMA Netw Open. 2023 Oct 2;6(10):e2339355. doi: 10.1001/jamanetworkopen.2023.39355. JAMA Netw Open. 2023. PMID: 37874566 Free PMC article.
-
Characteristics and Timing of Initial Virus Shedding in Severe Acute Respiratory Syndrome Coronavirus 2, Utah, USA.Emerg Infect Dis. 2021 Feb;27(2):352-359. doi: 10.3201/eid2702.203517. Epub 2020 Dec 4. Emerg Infect Dis. 2021. PMID: 33275874 Free PMC article. Review.
Cited by
-
Transmissibility of SARS-CoV-2 B.1.1.214 and Alpha Variants during 4 COVID-19 Waves, Kyoto, Japan, January 2020-June 2021.Emerg Infect Dis. 2022 Aug;28(8):1569-77. doi: 10.3201/eid2808.220420. Epub 2022 Jun 16. Emerg Infect Dis. 2022. PMID: 35710464 Free PMC article.
-
Serum neutralizing capacity and T-cell response against the omicron BA.1 variant in seropositive children and their parents one year after SARS-CoV-2 infection.Front Pediatr. 2023 Mar 27;11:1020865. doi: 10.3389/fped.2023.1020865. eCollection 2023. Front Pediatr. 2023. PMID: 37051428 Free PMC article.
-
Predictors of Severe Acute Respiratory Syndrome Coronavirus 2 Seropositivity Before Coronavirus Disease 2019 Vaccination Among Children 0-4 Years and Their Household Members in the SEARCh Study.Open Forum Infect Dis. 2022 Sep 30;9(10):ofac507. doi: 10.1093/ofid/ofac507. eCollection 2022 Oct. Open Forum Infect Dis. 2022. PMID: 36324323 Free PMC article.
-
Long COVID symptoms in exposed and infected children, adolescents and their parents one year after SARS-CoV-2 infection: A prospective observational cohort study.EBioMedicine. 2022 Oct;84:104245. doi: 10.1016/j.ebiom.2022.104245. Epub 2022 Sep 22. EBioMedicine. 2022. PMID: 36155957 Free PMC article.
-
High antibody levels and reduced cellular response in children up to one year after SARS-CoV-2 infection.Nat Commun. 2022 Nov 28;13(1):7315. doi: 10.1038/s41467-022-35055-1. Nat Commun. 2022. PMID: 36437276 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
