

Costs and staffing resource requirements for adaptive clinical trials: quantitative and qualitative results from the Costing Adaptive Trials project
- PMID: 34696781
- PMCID: PMC8545558
- DOI: 10.1186/s12916-021-02124-z
Costs and staffing resource requirements for adaptive clinical trials: quantitative and qualitative results from the Costing Adaptive Trials project
Abstract
Background: Adaptive designs offer great promise in improving the efficiency and patient-benefit of clinical trials. An important barrier to further increased use is a lack of understanding about which additional resources are required to conduct a high-quality adaptive clinical trial, compared to a traditional fixed design. The Costing Adaptive Trials (CAT) project investigated which additional resources may be required to support adaptive trials.
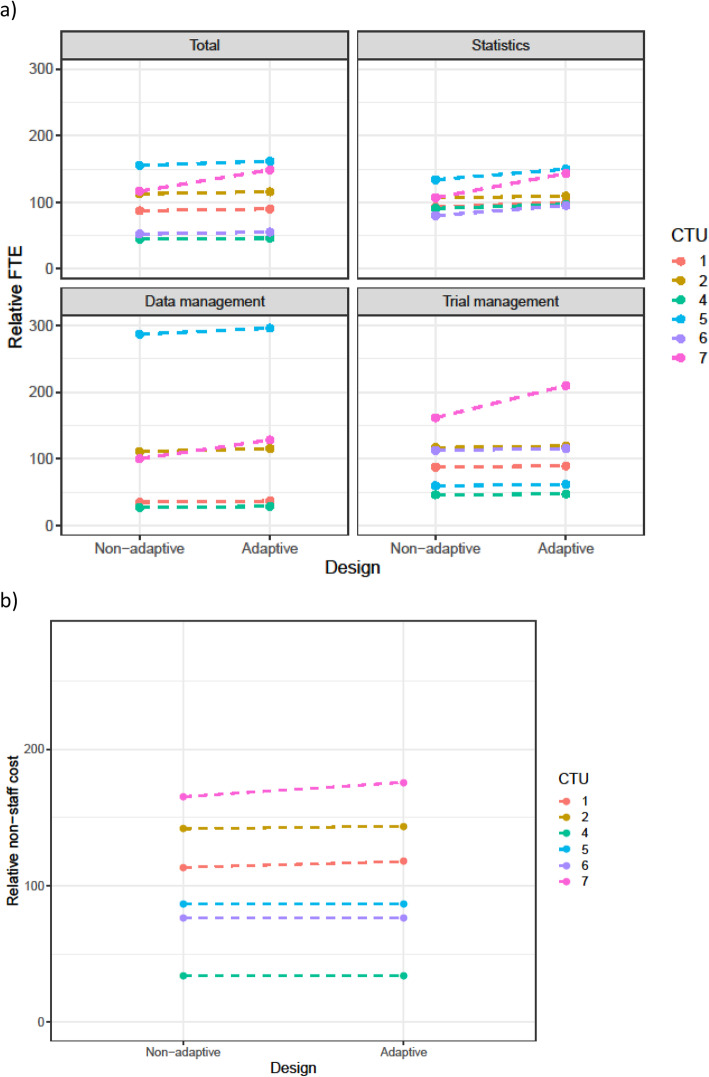
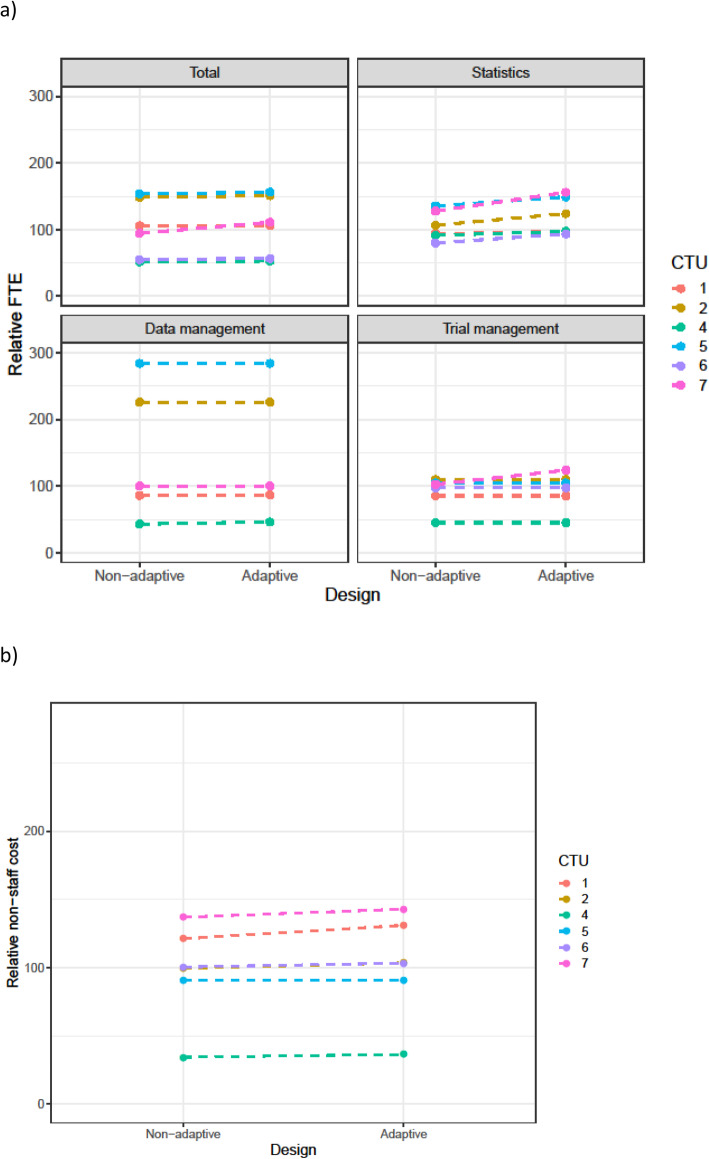
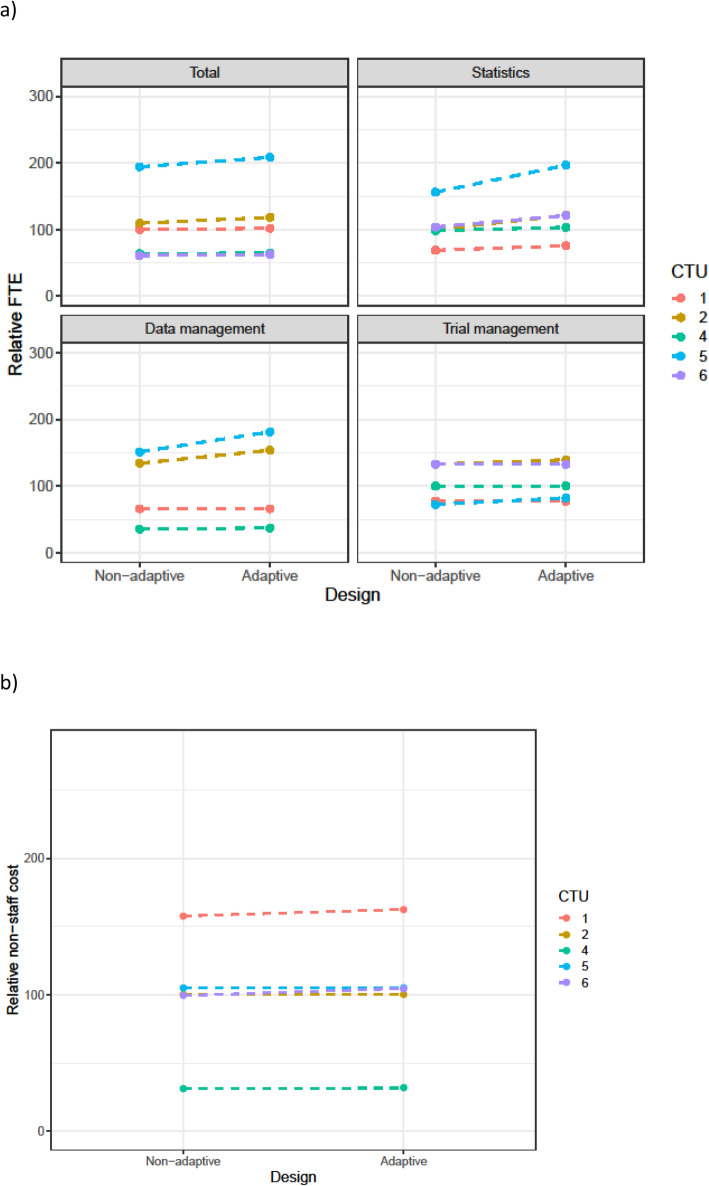
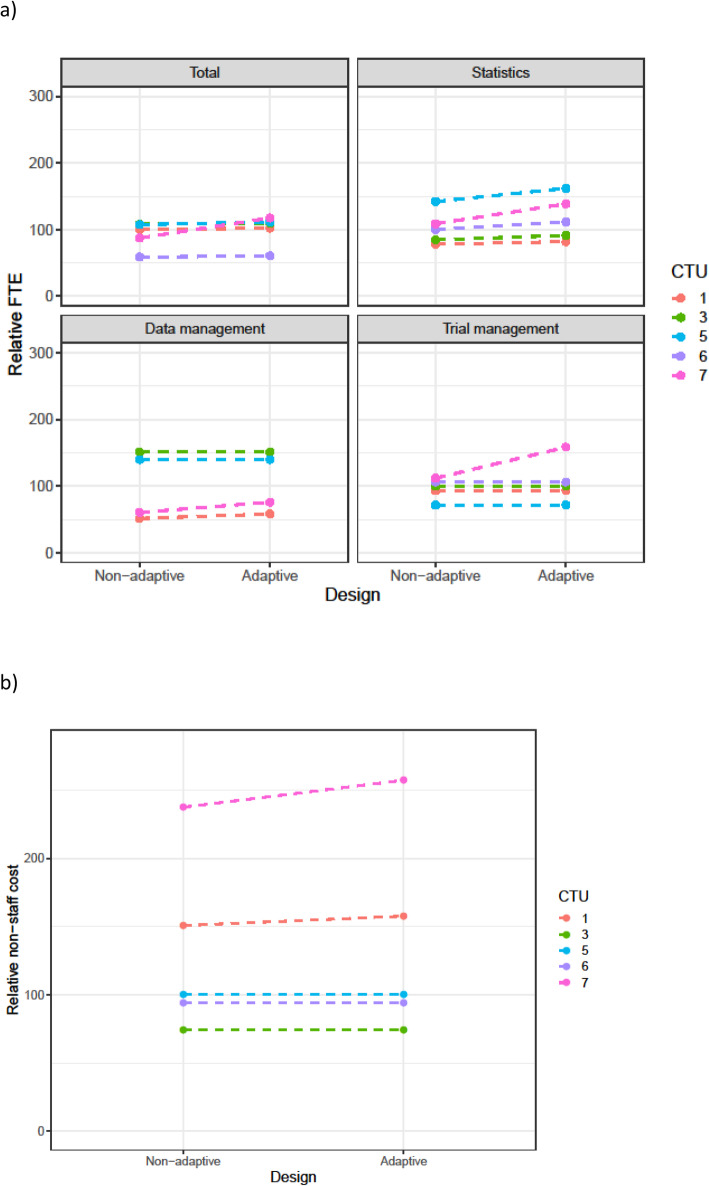
Methods: We conducted a mock costing exercise amongst seven Clinical Trials Units (CTUs) in the UK. Five scenarios were developed, derived from funded clinical trials, where a non-adaptive version and an adaptive version were described. Each scenario represented a different type of adaptive design. CTU staff were asked to provide the costs and staff time they estimated would be needed to support the trial, categorised into specified areas (e.g. statistics, data management, trial management). This was calculated separately for the non-adaptive and adaptive version of the trial, allowing paired comparisons. Interviews with 10 CTU staff who had completed the costing exercise were conducted by qualitative researchers to explore reasons for similarities and differences.
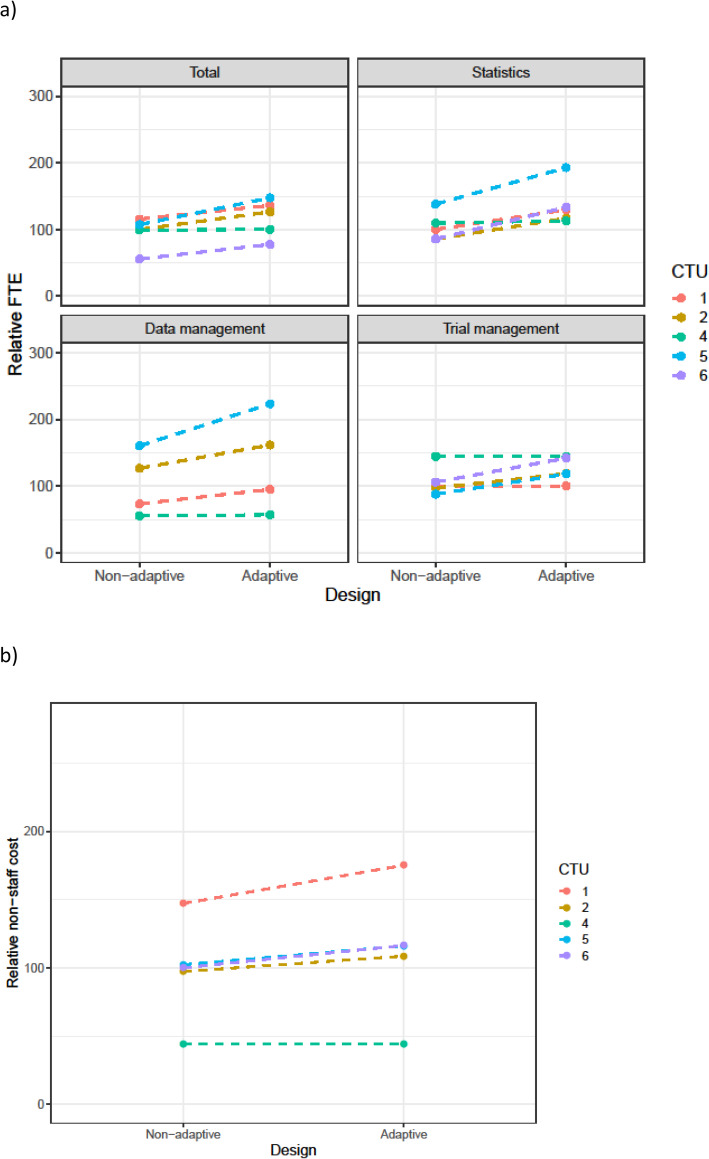
Results: Estimated resources associated with conducting an adaptive trial were always (moderately) higher than for the non-adaptive equivalent. The median increase was between 2 and 4% for all scenarios, except for sample size re-estimation which was 26.5% (as the adaptive design could lead to a lengthened study period). The highest increase was for statistical staff, with lower increases for data management and trial management staff. The percentage increase in resources varied across different CTUs. The interviews identified possible explanations for differences, including (1) experience in adaptive trials, (2) the complexity of the non-adaptive and adaptive design, and (3) the extent of non-trial specific core infrastructure funding the CTU had.
Conclusions: This work sheds light on additional resources required to adequately support a high-quality adaptive trial. The percentage increase in costs for supporting an adaptive trial was generally modest and should not be a barrier to adaptive designs being cost-effective to use in practice. Informed by the results of this research, guidance for investigators and funders will be developed on appropriately resourcing adaptive trials.
Keywords: Adaptive clinical trials; Adaptive designs; Clinical trials; Efficiency; Resource requirements; Trial coordination.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests that are relevant to this work.
Figures
References
-
- Pallmann P, Bedding AW, Choodari-Oskooei B, Dimairo M, Flight L, Hampson LV, Holmes J, Mander AP, Odondi L’, Sydes MR, Villar SS, Wason JMS, Weir CJ, Wheeler GM, Yap C, Jaki T. Adaptive designs in clinical trials: why use them, and how to run and report them. BMC Med. 2018;16(1):1–15. doi: 10.1186/s12916-018-1017-7. - DOI - PMC - PubMed
-
- Dimairo M, Pallmann P, Wason J, Todd S, Jaki T, Julious SA, Mander AP, Weir CJ, Koenig F, Walton MK, Nicholl JP, Coates E, Biggs K, Hamasaki T, Proschan MA, Scott JA, Ando Y, Hind D, Altman DG. The Adaptive designs CONSORT Extension (ACE) statement: a checklist with explanation and elaboration guideline for reporting randomised trials that use an adaptive design. BMJ. 2020;369:m115. doi: 10.1136/bmj.m115. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
