

Diabetes, hypertension, body mass index, smoking and COVID-19-related mortality: a systematic review and meta-analysis of observational studies
- PMID: 34697120
- PMCID: PMC8557249
- DOI: 10.1136/bmjopen-2021-052777
Diabetes, hypertension, body mass index, smoking and COVID-19-related mortality: a systematic review and meta-analysis of observational studies
Abstract
Objectives: We conducted a systematic literature review and meta-analysis of observational studies to investigate the association between diabetes, hypertension, body mass index (BMI) or smoking with the risk of death in patients with COVID-19 and to estimate the proportion of deaths attributable to these conditions.
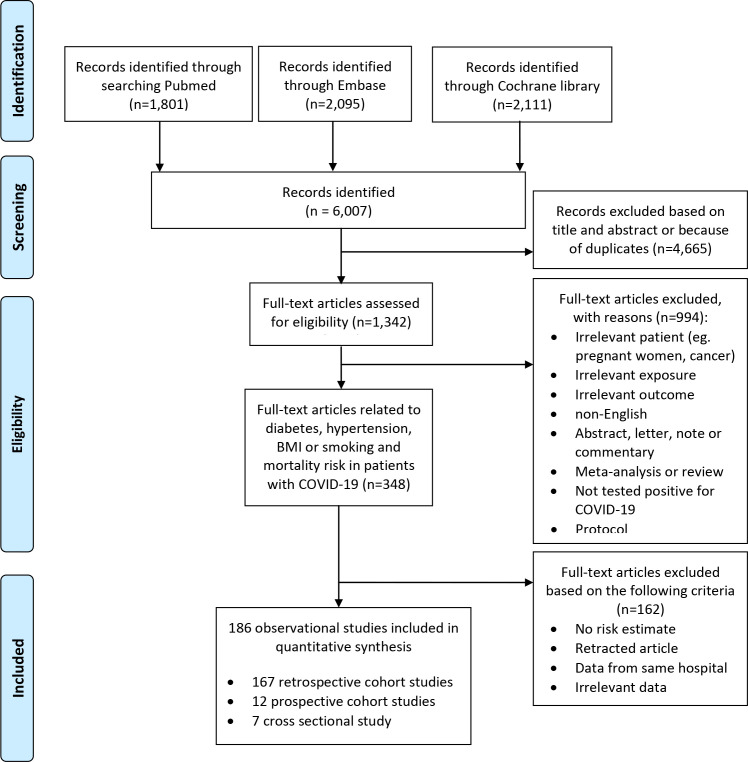
Methods: Relevant observational studies were identified by searches in the PubMed, Cochrane library and Embase databases through 14 November 2020. Random-effects models were used to estimate summary relative risks (SRRs) and 95% CIs. Certainty of evidence was assessed using the Cochrane methods and the Grading of Recommendations, Assessment, Development and Evaluations framework.
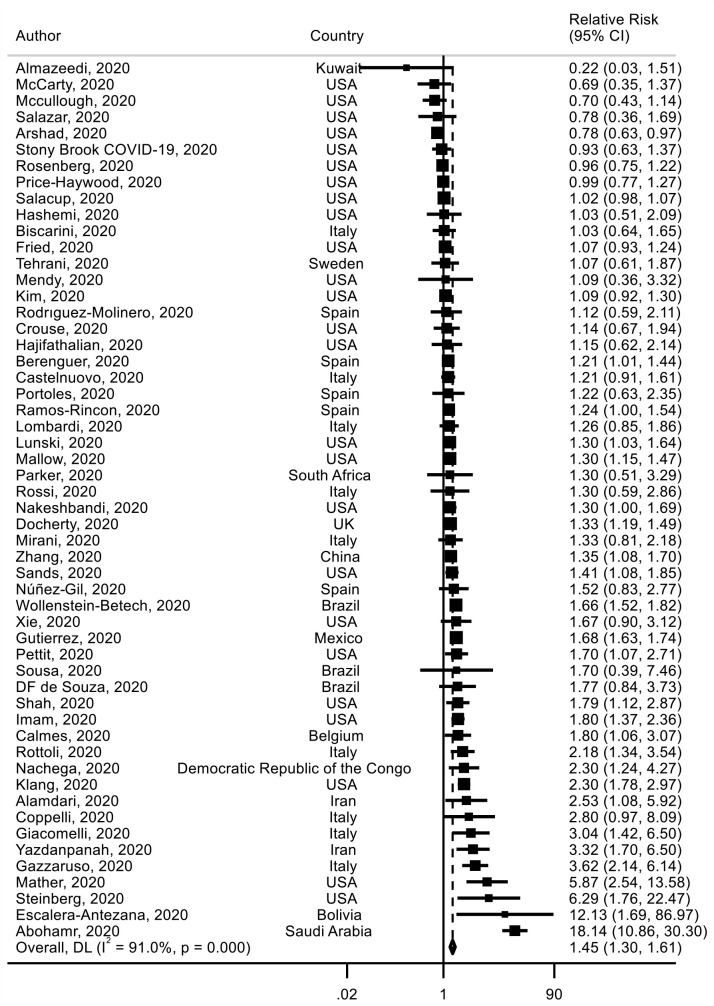
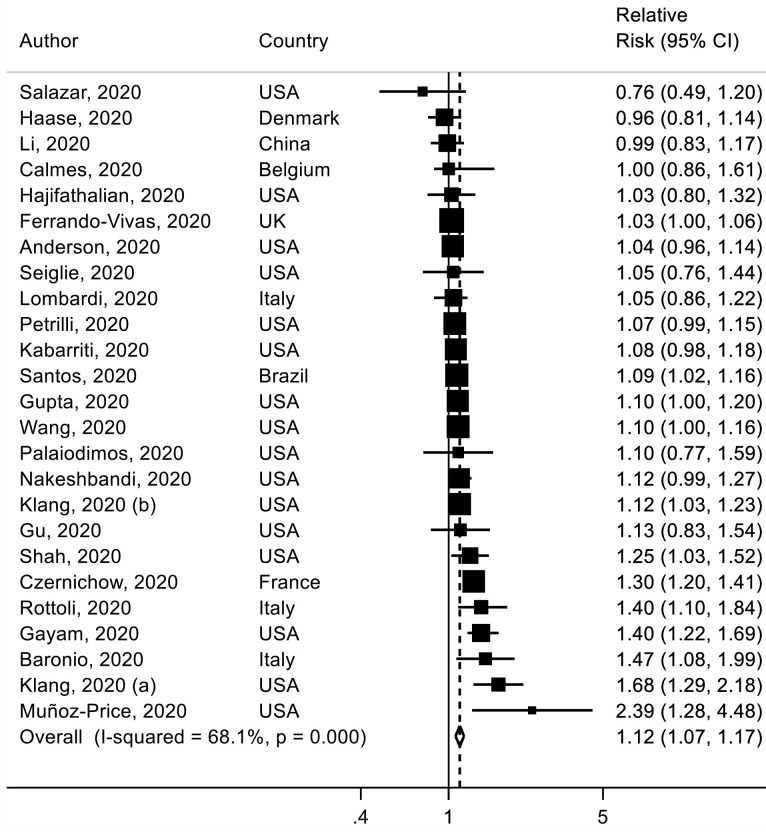
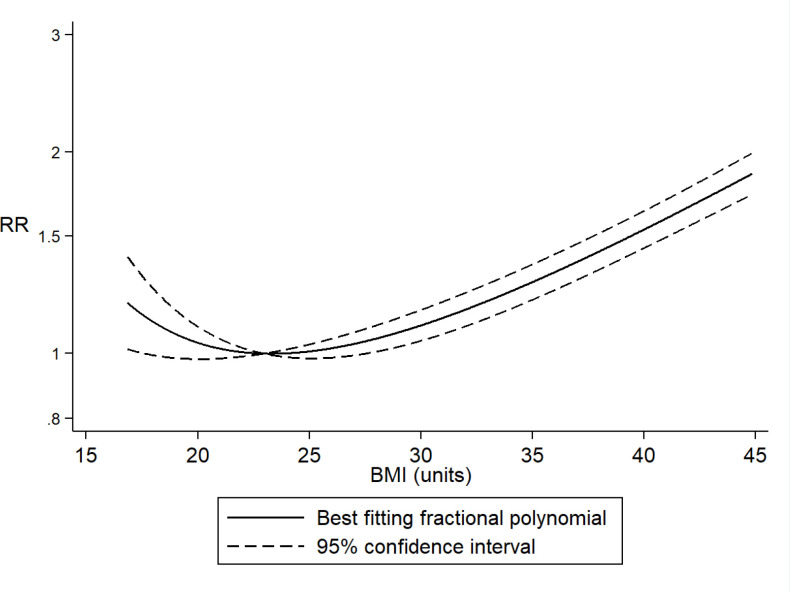
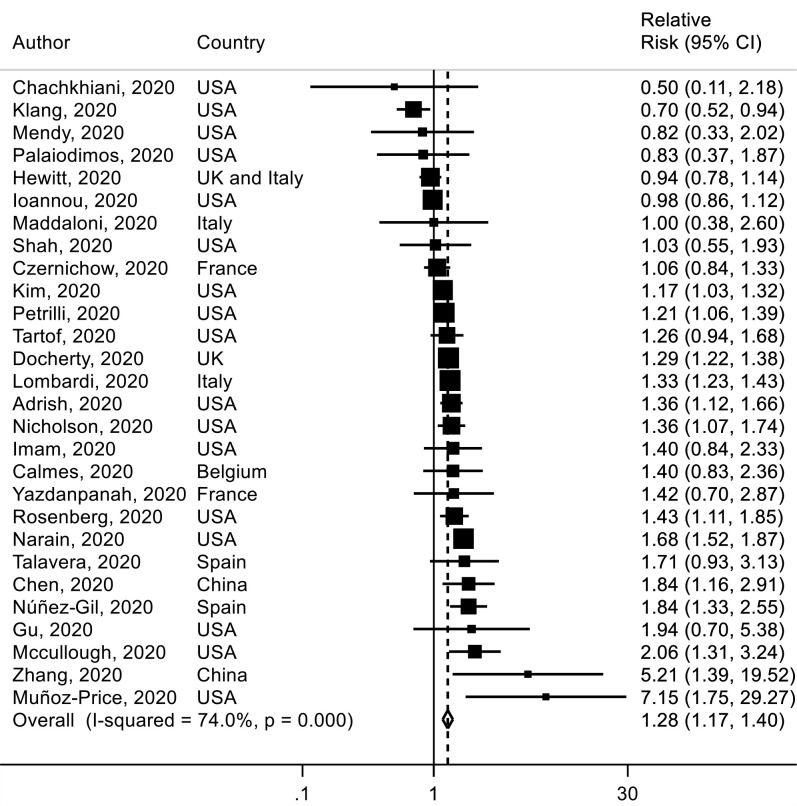
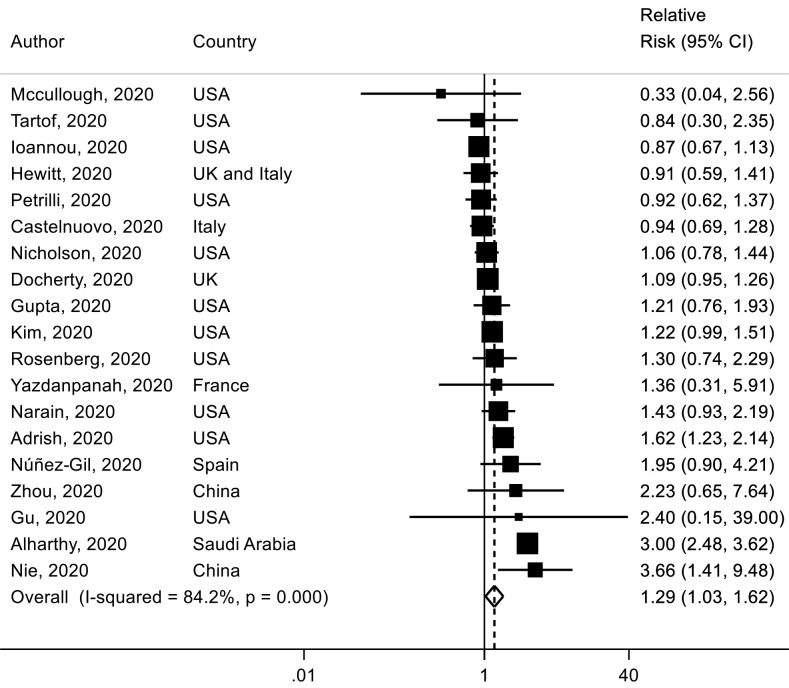
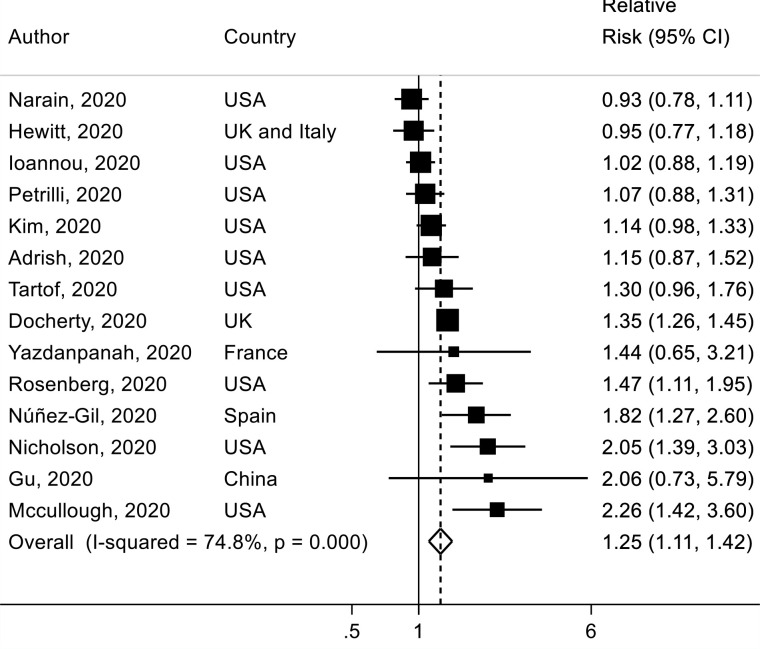
Results: A total of 186 studies representing 210 447 deaths among 1 304 587 patients with COVID-19 were included in this analysis. The SRR for death in patients with COVID-19 was 1.54 (95% CI 1.44 to 1.64, I2=92%, n=145, low certainty) for diabetes and 1.42 (95% CI 1.30 to 1.54, I2=90%, n=127, low certainty) for hypertension compared with patients without each of these comorbidities. Regarding obesity, the SSR was 1.45 (95% CI 1.31 to 1.61, I2=91%, n=54, high certainty) for patients with BMI ≥30 kg/m2 compared with those with BMI <30 kg/m2 and 1.12 (95% CI 1.07 to 1.17, I2=68%, n=25) per 5 kg/m2 increase in BMI. There was evidence of a J-shaped non-linear dose-response relationship between BMI and mortality from COVID-19, with the nadir of the curve at a BMI of around 22-24, and a 1.5-2-fold increase in COVID-19 mortality with extreme obesity (BMI of 40-45). The SRR was 1.28 (95% CI 1.17 to 1.40, I2=74%, n=28, low certainty) for ever, 1.29 (95% CI 1.03 to 1.62, I2=84%, n=19) for current and 1.25 (95% CI 1.11 to 1.42, I2=75%, n=14) for former smokers compared with never smokers. The absolute risk of COVID-19 death was increased by 14%, 11%, 12% and 7% for diabetes, hypertension, obesity and smoking, respectively. The proportion of deaths attributable to diabetes, hypertension, obesity and smoking was 8%, 7%, 11% and 2%, respectively.
Conclusion: Our findings suggest that diabetes, hypertension, obesity and smoking were associated with higher COVID-19 mortality, contributing to nearly 30% of COVID-19 deaths.
Trial registration number: CRD42020218115.
Keywords: COVID-19; epidemiology; general diabetes; hypertension.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO . Coronavirus disease (COVID-19) pandemic, 2020. Available: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=Cj...
-
- World Health Organization (WHO) . Who coronavirus disease (COVID-19) Dashboard. Available: https://covid19.who.int/?gclid=CjwKCAiA57D_BRAZEiwAZcfCxWQWth4sNqEZ1J34K...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical