

CSF Findings in Acute NMDAR and LGI1 Antibody-Associated Autoimmune Encephalitis
- PMID: 34697224
- PMCID: PMC8546742
- DOI: 10.1212/NXI.0000000000001086
CSF Findings in Acute NMDAR and LGI1 Antibody-Associated Autoimmune Encephalitis
Abstract
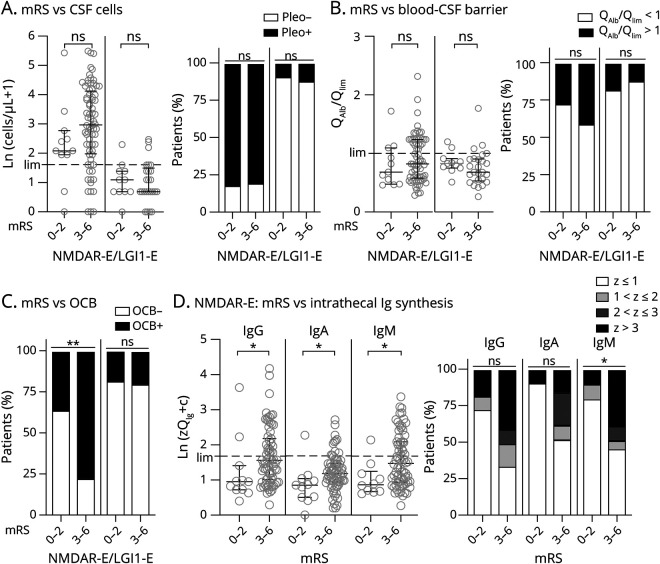
Background and objectives: CSF in antibody-defined autoimmune encephalitis (AE) subtypes shows subtype-dependent degrees of inflammation ranging from rare and often mild to frequent and often robust. AEs with NMDA receptor antibodies (NMDAR-E) and leucine-rich glioma-inactivated protein 1 antibodies (LGI1-E) represent opposite ends of this spectrum: NMDAR-E with typically frequent/robust and LGI1-E with rare/mild CSF inflammation. For a more in-depth analysis, we characterized CSF findings in acute, therapy-naive NMDAR-E and LGI1-E in a multicentric, retrospective, cross-sectional setting.
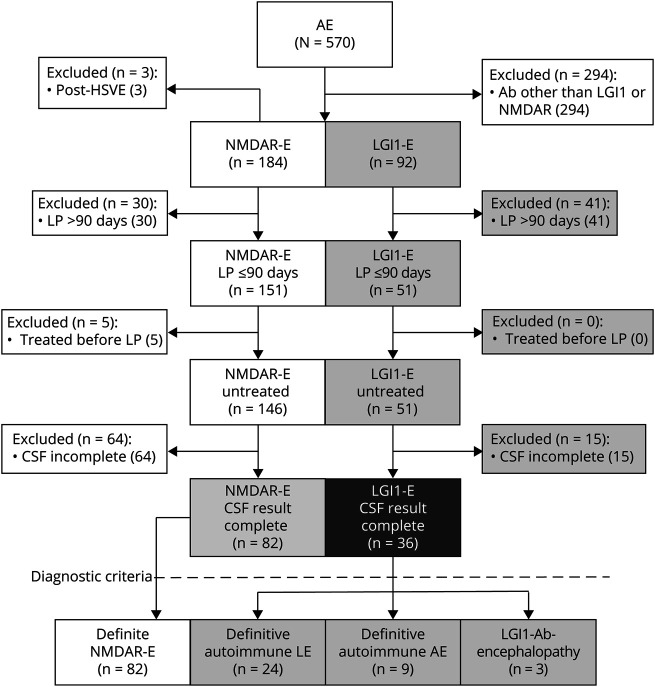
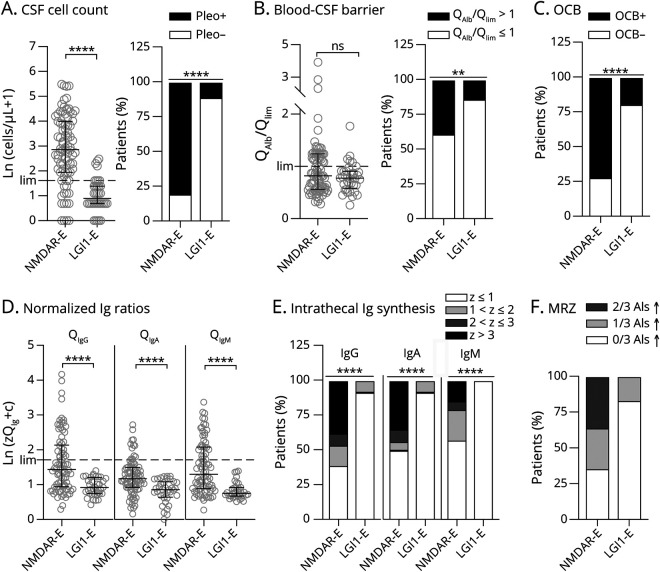
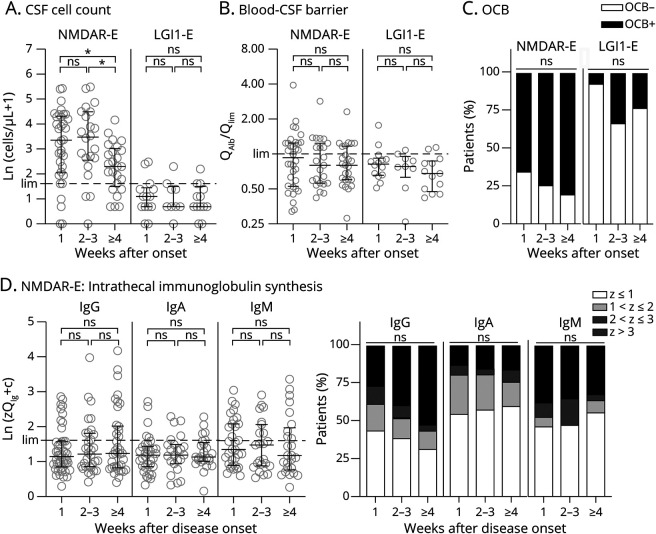
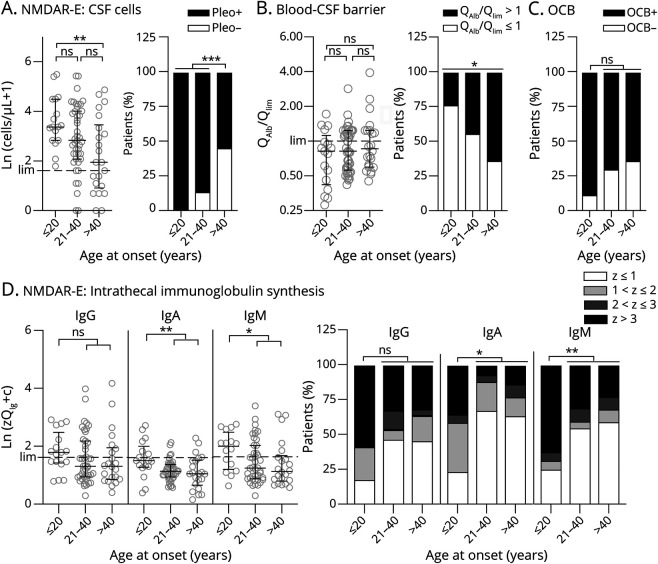
Methods: Eighty-two patients with NMDAR-E and 36 patients with LGI1-E from the GErman NEtwork for Research of AuToimmune Encephalitis (GENERATE) with lumbar puncture within 90 days of onset and before immunotherapy were included. CSF parameters comprised leukocytes, oligoclonal bands (OCBs), and CSF/serum ratios for albumin, immunoglobulin G (IgG), A (IgA), and M (IgM), the latter 3 converted to Z scores according to Reiber formulas. The MRZ reaction was tested in 14 patients with NMDAR-E and 6 patients with LGI1-E, respectively.
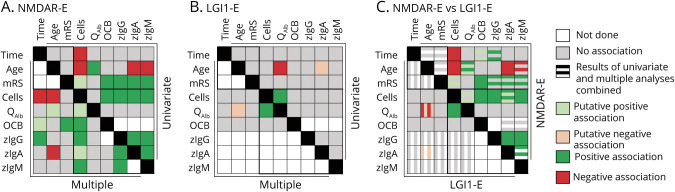
Results: CSF was abnormal in 94% of NMDAR-E but only in 36% of LGI1-E patients. Robust quantitative intrathecal immunoglobulin synthesis (IIS, IgG > IgM >> IgA) was characteristic for NMDAR-E, but absent in LGI-E. In NMDAR-E, CSF leukocytes were higher when IIS was present or more pronounced. In addition, in NMDAR-E, CSF leukocytes were lower and IIS occurred less often and if so to a lesser degree at older age. Patients with NMDAR-E with severe functional impairment more often had positive OCBs. In CSF obtained later than 3 weeks of onset, leukocytes were lower. In parallel, the correlation of leukocytes with IIS disappeared as IIS was partially independent of disease duration. The MRZ reaction was positive in 5 (36%) patients with NMDAR-E. All these associations were completely absent in LGI1-E. Here, younger patients showed more blood-CSF barrier dysfunction. In LGI1-E, but not in NMDAR-E, the blood-CSF barrier was more dysfunctional when CSF leukocytes were higher.
Discussion: NMDAR-E and LGI-E differ in their typical extent of CSF inflammation. In addition, the patterns formed by the different inflammatory CSF parameters and their relationship with disease severity, age, and disease duration are subtype-characteristic. Moreover, signs for multiple sclerosis-like chronic inflammation are present in a subgroup of patients with NMDAR-E. These CSF patterns might be markers for the different immunopathogeneses of LGI1-E and NMDAR-E.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10(12):835-44. - PubMed
-
- van Sonderen A, Schreurs MW, Wirtz PW, Sillevis Smitt PA, Titulaer MJ. From VGKC to LGI1 and Caspr2 encephalitis: the evolution of a disease entity over time. Autoimmun Rev. 2016;15(10):970-974. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous