

Platypnea Orthodeoxia Due to a Patent Foramen Ovale and Intrapulmonary Shunting After Severe COVID-19 Pneumonia
- PMID: 34697281
- PMCID: PMC8559663
- DOI: 10.12659/AJCR.933975
Platypnea Orthodeoxia Due to a Patent Foramen Ovale and Intrapulmonary Shunting After Severe COVID-19 Pneumonia
Abstract
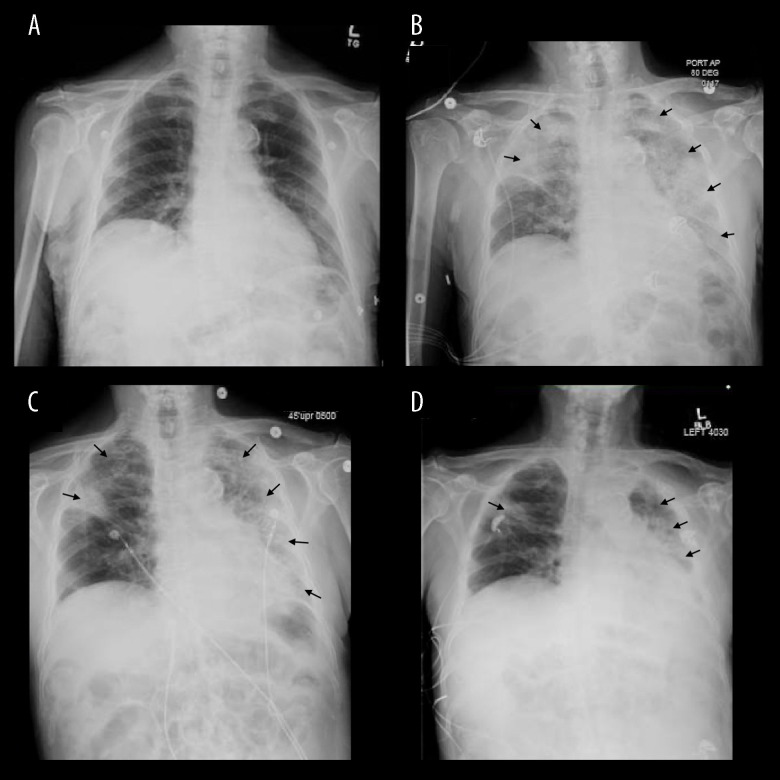
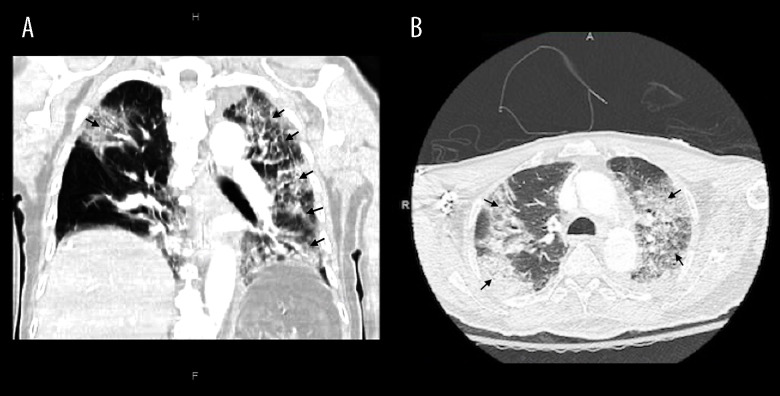
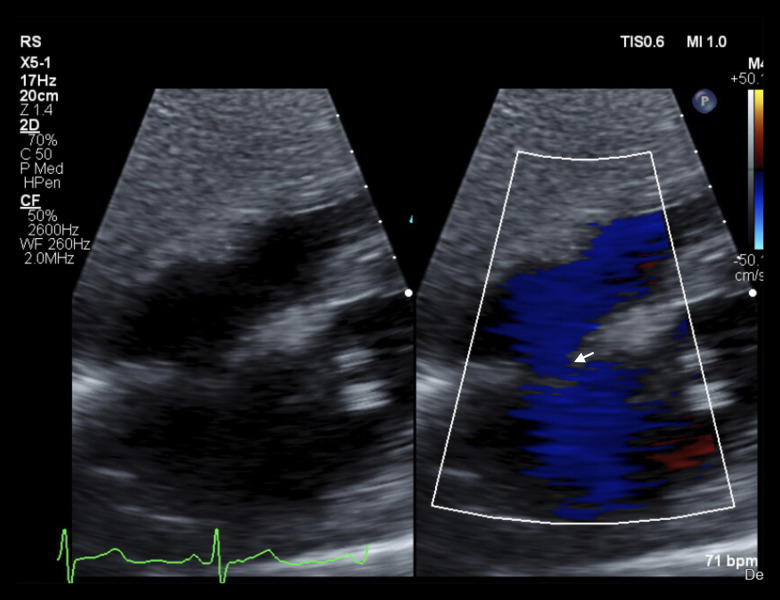
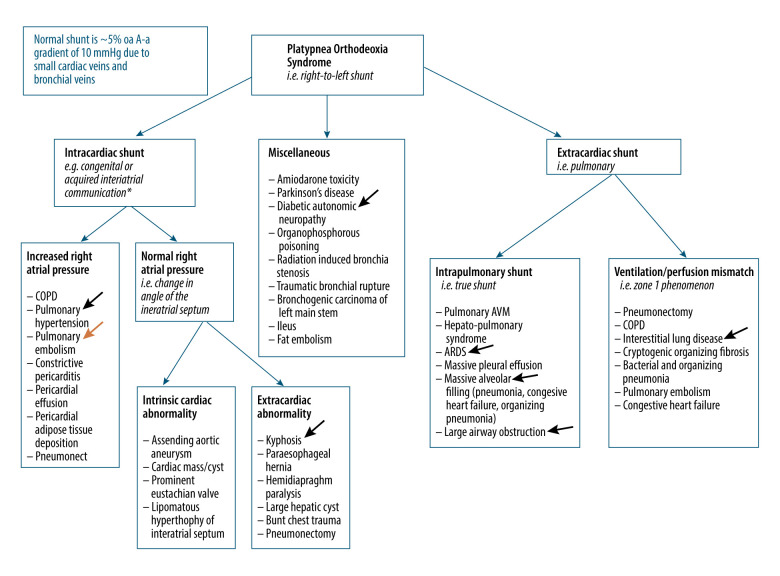
BACKGROUND Platypnea orthodeoxia syndrome (POS) presents with positional dyspnea and hypoxemia defined as arterial desaturation of at least 5% or a drop in PaO2 of at least 4 mmHg. Causes of POS include a variety of cardiopulmonary etiologies and has been reported in patients recovering from severe COVID-19 pneumonia. However, clinical presentation and outcomes in a patient with multiple interrelated mechanisms of shunting has not been documented. CASE REPORT An 85-year-old man hospitalized for hypertensive emergency and severe COVID-19 pneumonia was diagnosed with platypnea orthodeoxia on day 28 of illness. During his disease course, the patient required supplemental oxygen by high-flow nasal cannula but never required invasive mechanical ventilation. Chest imaging revealed evolving mixed consolidation and ground-glass opacities with a patchy and diffuse distribution, involving most of the left lung. Echocardiography was ordered to evaluate for intracardiac shunt, which revealed a patent foramen ovale. Closure of the patent foramen ovale was not pursued. Management included graded progression to standing and supplemental oxygen increases when upright. The patient was discharged to a skilled nursing facility and his positional oxygen requirement resolved on approximately day 78. CONCLUSIONS The present case highlights the multiple interrelated mechanisms of shunting in patients with COVID-related lung disease and a patent foramen ovale. Eight prior cases of POS after COVID-19 pneumonia have been reported to date but none with a known patent foramen ovale. In patients with persistent positional oxygen requirements at follow-up, quantifying shunt fraction over time through multiple modalities can guide treatment decisions.
Conflict of interest statement
Figures
References
-
- Agrawal A, Palkar A, Talwar A. The multiple dimensions of platypnea-orthodeoxia syndrome: A review. Respir Med. 2017;129:31–38. - PubMed
-
- Akin E, Krüger U, Braun P, et al. The platypnea-orthodeoxia syndrome. Eur Rev Med Pharmacol Sci. 2014;18(18):2599–604. - PubMed
-
- Gadre A, Highland KB, Mehta A. Reversible platypnea-orthodeoxia syndrome from ventilation-perfusion mismatch in interstitial lung disease: A novel etiology. Ann Am Thorac Soc. 2016;13(1):137–38. - PubMed
-
- Bellato V, Brusa S, Balazova J, et al. Platypnea-orthodeoxia syndrome in interatrial right to left shunt postpneumonectomy. Minerva Anestesiol. 2008;74(6):271–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
