

The Distribution of Multidrug-resistant Microorganisms and Treatment Status of Hospital-acquired Pneumonia/Ventilator-associated Pneumonia in Adult Intensive Care Units: a Prospective Cohort Observational Study
- PMID: 34697926
- PMCID: PMC8546312
- DOI: 10.3346/jkms.2021.36.e251
The Distribution of Multidrug-resistant Microorganisms and Treatment Status of Hospital-acquired Pneumonia/Ventilator-associated Pneumonia in Adult Intensive Care Units: a Prospective Cohort Observational Study
Abstract
Background: It is essential to determine the distribution of the causative microorganisms in the region and the status of local antibiotic resistance for the proper treatment of hospital-acquired pneumonia/ventilator-associated pneumonia (HAP/VAP). This study aimed to investigate the occurrence and causative strains of HAP/VAP, distribution of resistant bacteria, use of antibiotics, and the ensuing outcomes of patients in Korea.
Methods: A multicenter prospective observational cohort study was conducted among patients with HAP/VAP admitted to the medical intensive care unit of 5 tertiary referral centers between August 2012 and June 2015. Patients' demographic and clinical data were collected.
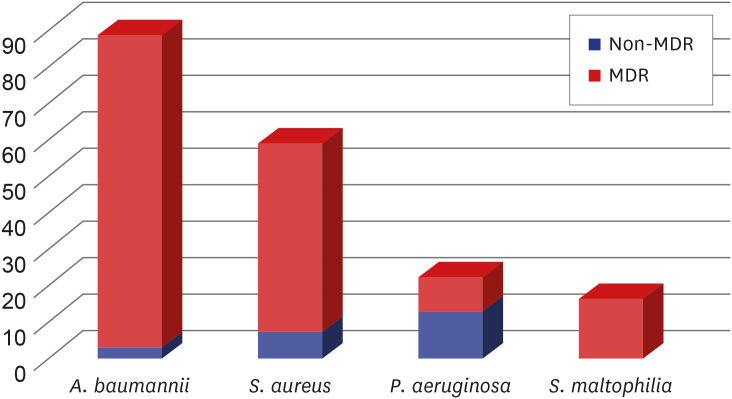
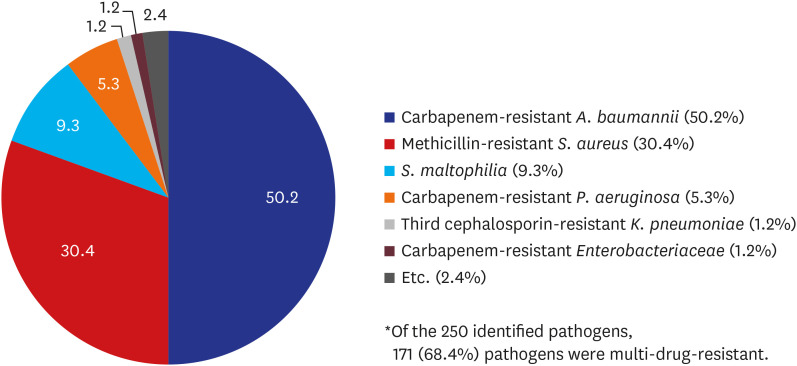
Results: A total of 381 patients were diagnosed with HAP/VAP. Their median age was 69 (59-76) years and 71% were males. A majority of the patients (88%) had late-onset (> 5 days) HAP/VAP. One-quarter of the patients (n = 99) had at least one risk factor for multidrug-resistant (MDR) pathogens, such as prior intravenous antibiotic use within the last 90 days. Microbiological specimens were mostly obtained noninvasively (87%) using sputum or endotracheal aspirates. Pathogens were identified in 235 (62%) of the 381 patients. The most common bacterial pathogen was Acinetobacter baumannii (n = 89), followed by Staphylococcus aureus (n = 52), Klebsiella pneumoniae (n = 25) and Pseudomonas aeruginosa (n = 22). Most of isolated A. baumannii (97%) and S. aureus (88%) were multidrug resistant. The most commonly used empirical antibiotic regimens were carbapenem-based antibiotics (38%), followed by extended-spectrum penicillin/β-lactamase inhibitor (34%). Glycopeptide or linezolid were also used in combination in 54% of patients. The 28-day mortality rate of the patients with HAP/VAP was 30% and the 60-day mortality was 46%. Patients who used empirical antibiotics appropriately had significantly lower mortality rates than those who did not (28-day mortality: 25% vs. 40%, P = 0.032; 60-day mortality: 41% vs. 55%, P = 0.032, respectively). Administration of appropriate empirical antibiotics (odds ratio [OR], 0.282; confidence interval [CI], 0.092-0.859; P = 0.026), Day 7 treatment failure (OR, 4.515; CI, 1.545-13.192; P = 0.006), and APACHE II score on day 1 (OR, 1.326; CI, 0.988-1.779; P = 0.012) were the factors that determined the 28-day mortality in patients with HAP who had identified bacteria as pathogens.
Conclusion: In HAP/VAP patients, there was a large burden of MDR pathogens, and their associated mortality rate was high. Proper selection of empirical antibiotics was significantly associated with the patient's prognosis; however, there was a discrepancy between major pathogens and empirical antibiotic therapy.
Keywords: Drug Resistance, Bacterial; Healthcare-associated Pneumonia; Intensive Care Units; Treatment Outcome; Ventilator-associated Pneumonia.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Hospital-acquired pneumonia and ventilator-associated pneumonia in adults at Siriraj Hospital: etiology, clinical outcomes, and impact of antimicrobial resistance.J Med Assoc Thai. 2010 Jan;93 Suppl 1:S126-38. J Med Assoc Thai. 2010. PMID: 20364567
-
Microorganisms and clinical outcomes of early- and late-onset ventilator-associated pneumonia at Srinagarind Hospital, a tertiary center in Northeastern Thailand.BMC Pulm Med. 2021 Jan 30;21(1):47. doi: 10.1186/s12890-021-01415-8. BMC Pulm Med. 2021. PMID: 33516213 Free PMC article.
-
Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality.Medicina (Kaunas). 2019 Feb 13;55(2):49. doi: 10.3390/medicina55020049. Medicina (Kaunas). 2019. PMID: 30781896 Free PMC article.
-
[Guidelines for treatment of pneumonia in intensive care units].Infez Med. 2005;Suppl:7-17. Infez Med. 2005. PMID: 16801748 Review. Italian.
-
Disease burden of intensive care unit-acquired pneumonia in China: a systematic review and meta-analysis.Int J Infect Dis. 2014 Dec;29:84-90. doi: 10.1016/j.ijid.2014.05.030. Epub 2014 Oct 24. Int J Infect Dis. 2014. PMID: 25449241
Cited by
-
Efficacy and safety of intravenous combined with aerosolised polymyxin versus intravenous polymyxin alone in the treatment of multidrug-resistant gram-negative bacterial pneumonia: A systematic review and meta-analysis.Heliyon. 2023 Apr 25;9(5):e15774. doi: 10.1016/j.heliyon.2023.e15774. eCollection 2023 May. Heliyon. 2023. PMID: 37159708 Free PMC article.
-
Distribution characteristics of aerosol microorganisms in bronchoscopy room and the risk assessment of nosocomial infection.Front Public Health. 2025 Apr 28;13:1556364. doi: 10.3389/fpubh.2025.1556364. eCollection 2025. Front Public Health. 2025. PMID: 40356821 Free PMC article.
-
Independent risk factors and outcomes for ventilator-associated pneumonia due to multidrug-resistant organisms after cardiac valvular surgery.Front Cardiovasc Med. 2025 Apr 3;12:1570195. doi: 10.3389/fcvm.2025.1570195. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40248251 Free PMC article.
-
Application of double-sleeve endotracheal tube in infection control for icu patients: a randomized controlled trial.Head Face Med. 2025 Feb 26;21(1):12. doi: 10.1186/s13005-025-00488-8. Head Face Med. 2025. PMID: 40011996 Free PMC article. Clinical Trial.
-
Characteristics of ventilator-associated pneumonia due to Gram-negative bacteria in the intensive care unit: A single-center experience.Medicine (Baltimore). 2025 Jun 27;104(26):e42946. doi: 10.1097/MD.0000000000042946. Medicine (Baltimore). 2025. PMID: 40587686 Free PMC article.
References
-
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. - PubMed
-
- Agrafiotis M, Siempos II, Ntaidou TK, Falagas ME. Attributable mortality of ventilator-associated pneumonia: a meta-analysis. Int J Tuberc Lung Dis. 2011;15(9):1154–1163. - PubMed
-
- Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. A novel algorithm to analyze epidemiology and outcomes of carbapenem resistance among patients with hospital-acquired and ventilator-associated pneumonia: a retrospective cohort study. Chest. 2019;155(6):1119–1130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
