

Validation of a visual analog scale for assessing cough severity in patients with chronic cough
- PMID: 34697975
- PMCID: PMC8552382
- DOI: 10.1177/17534666211049743
Validation of a visual analog scale for assessing cough severity in patients with chronic cough
Abstract
Introduction: Patients with chronic cough experience considerable burden. The cough severity visual analog scale (VAS) records patients' assessment of cough severity on a 100-mm linear scale ranging from "no cough" (0 mm) to "worst cough" (100 mm). Although cough severity scales are widely used in clinical practice and research, their use in patients with refractory or unexplained chronic cough has not been formally validated.
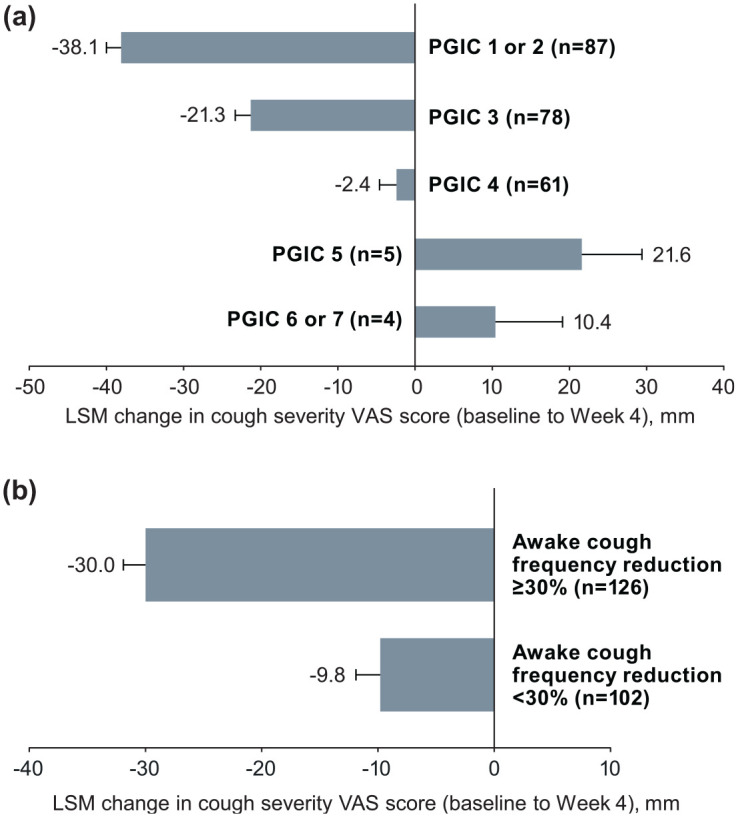
Methods: This analysis includes data from a phase 2b randomized controlled trial of the P2X3-receptor antagonist gefapixant for treatment of refractory or unexplained chronic cough (NCT02612610). Cough severity VAS scores were assessed at baseline and Weeks 4, 8, and 12. The cough severity VAS was validated using several outcomes, including the Cough Severity Diary (CSD), Leicester Cough Questionnaire (LCQ), patient global impression of change (PGIC) scale, and objective cough frequency. Validation metrics included test-retest reliability, convergent and known-groups validity, responsiveness, and score interpretation (i.e., clinically meaningful change threshold).
Results: The analysis included 253 patients (median age, 61.0 years; females, 76%). Test-retest reliability of the cough severity VAS was moderate (intraclass correlation coefficient, 0.51). The cough severity VAS had acceptable convergent validity with other related measures (Pearson r of 0.53 and -0.41 for CSD and LCQ total scores, respectively; p < 0.0001 for each). Known-groups validity was supported by significant differences in mean cough severity VAS scores across severity groups defined using CSD, LCQ, and cough frequency tertiles. A large effect size was observed in patients with the greatest improvements in PGIC (Cohen d = -1.8). A ⩾ 30-mm reduction in the cough severity VAS was estimated as a clinically meaningful change threshold for clinical trials in chronic cough.
Conclusions: The cough severity VAS is a valid and responsive measure. A cough severity VAS reduction of ⩾ 30 mm can discriminate clinically meaningful changes in chronic cough severity in clinical studies.
Keywords: Cough Severity Diary; Leicester Cough Questionnaire; clinically meaningful change; cough monitoring; idiopathic cough; minimal important difference; objective cough frequency; patient-reported outcomes; responder threshold.
Conflict of interest statement
Figures
References
-
- Song WJ, Chang YS, Faruqi S, et al. The global epidemiology of chronic cough in adults: a systematic review and meta-analysis. Eur Respir J 2015; 45: 1479–1481. - PubMed
-
- Çolak Y, Nordestgaard BG, Laursen LC, et al. Risk factors for chronic cough among 14,669 individuals from the general population. Chest 2017; 152: 563–573. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
