

Resistance Testing for Management of HIV Virologic Failure in Sub-Saharan Africa : An Unblinded Randomized Controlled Trial
- PMID: 34698502
- PMCID: PMC8688215
- DOI: 10.7326/M21-2229
Resistance Testing for Management of HIV Virologic Failure in Sub-Saharan Africa : An Unblinded Randomized Controlled Trial
Abstract
Background: Virologic failure in HIV predicts the development of drug resistance and mortality. Genotypic resistance testing (GRT), which is the standard of care after virologic failure in high-income settings, is rarely implemented in sub-Saharan Africa.
Objective: To estimate the effectiveness of GRT for improving virologic suppression rates among people with HIV in sub-Saharan Africa for whom first-line therapy fails.
Design: Pragmatic, unblinded, randomized controlled trial. (ClinicalTrials.gov: NCT02787499).
Setting: Ambulatory HIV clinics in the public sector in Uganda and South Africa.
Patients: Adults receiving first-line antiretroviral therapy with a recent HIV RNA viral load of 1000 copies/mL or higher.
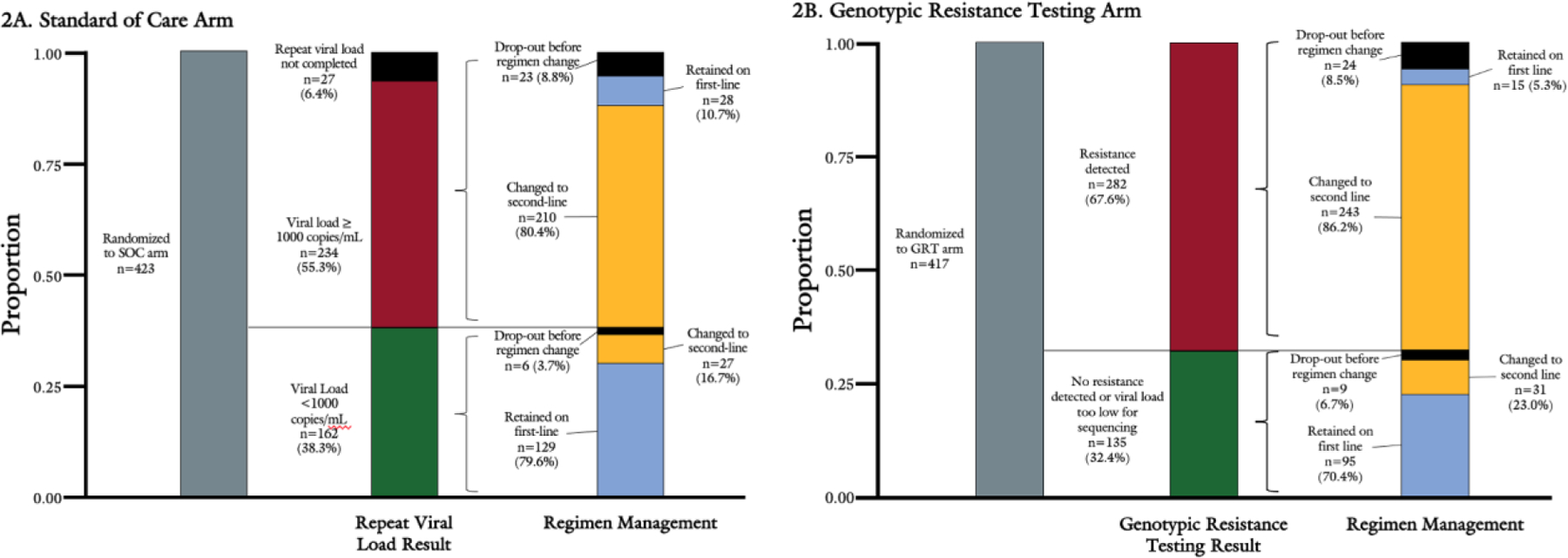
Intervention: Participants were randomly assigned to receive standard of care (SOC), including adherence counseling sessions and repeated viral load testing, or immediate GRT.
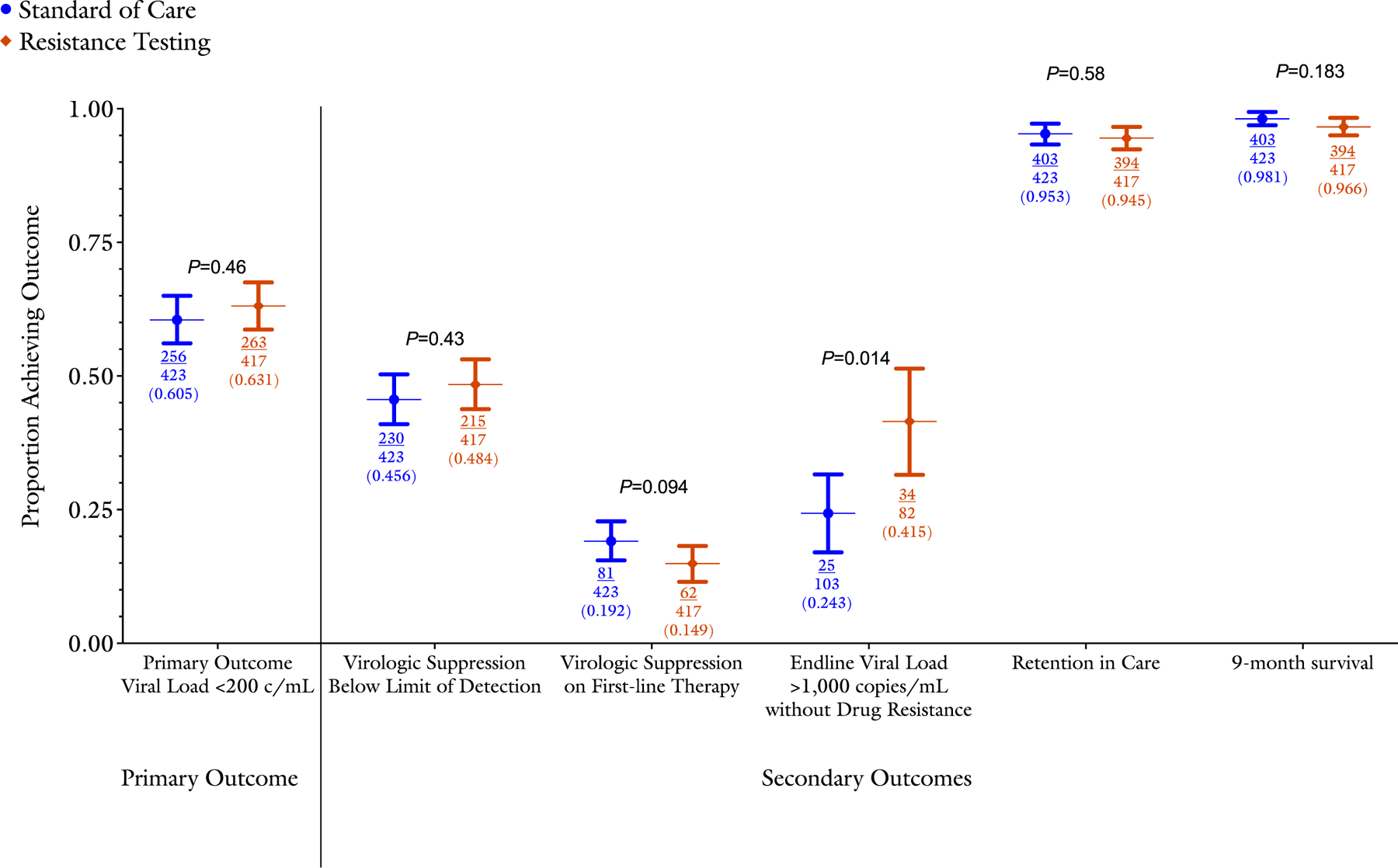
Measurements: The primary outcome of interest was achievement of an HIV RNA viral load below 200 copies/mL 9 months after enrollment.
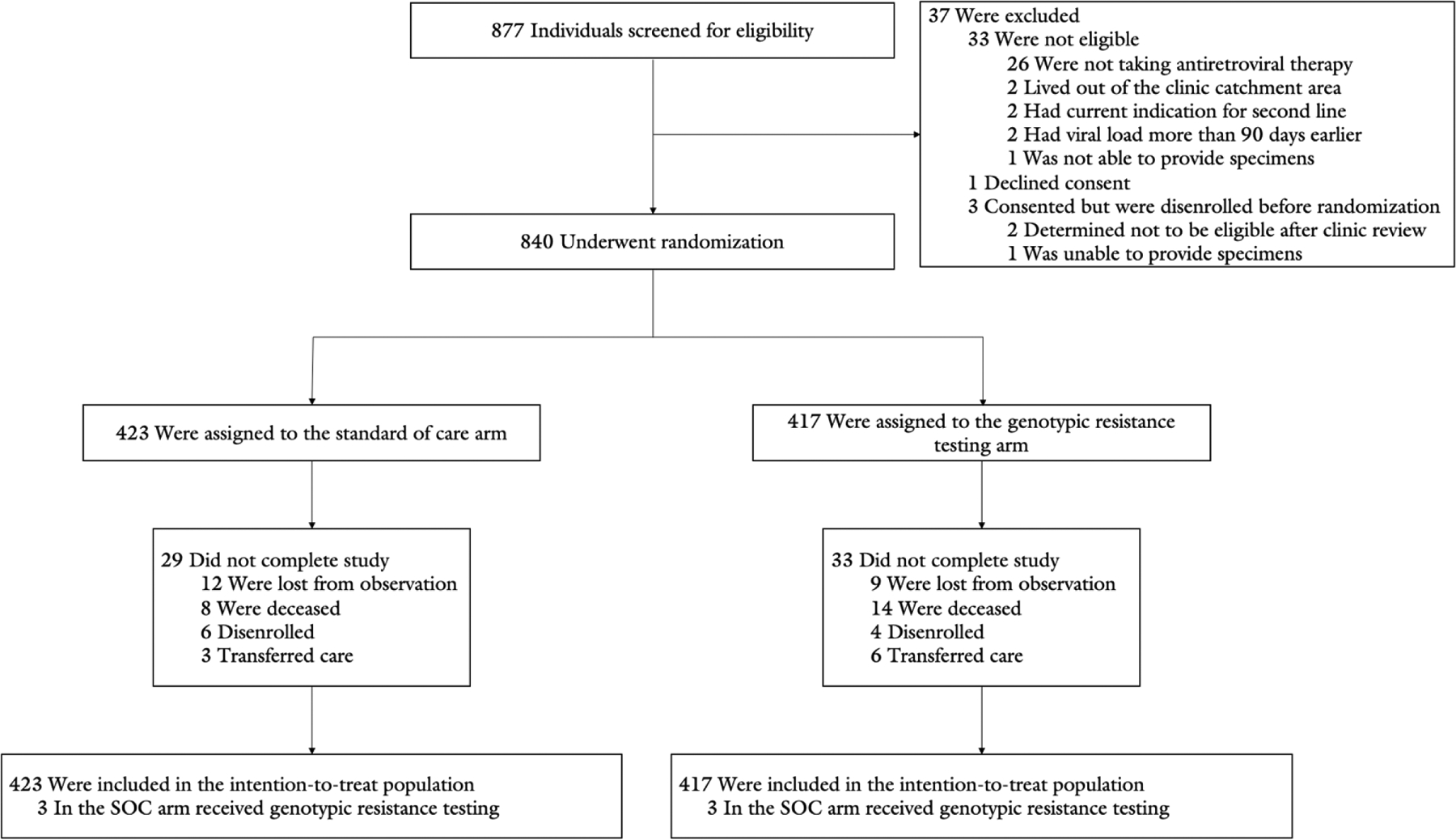
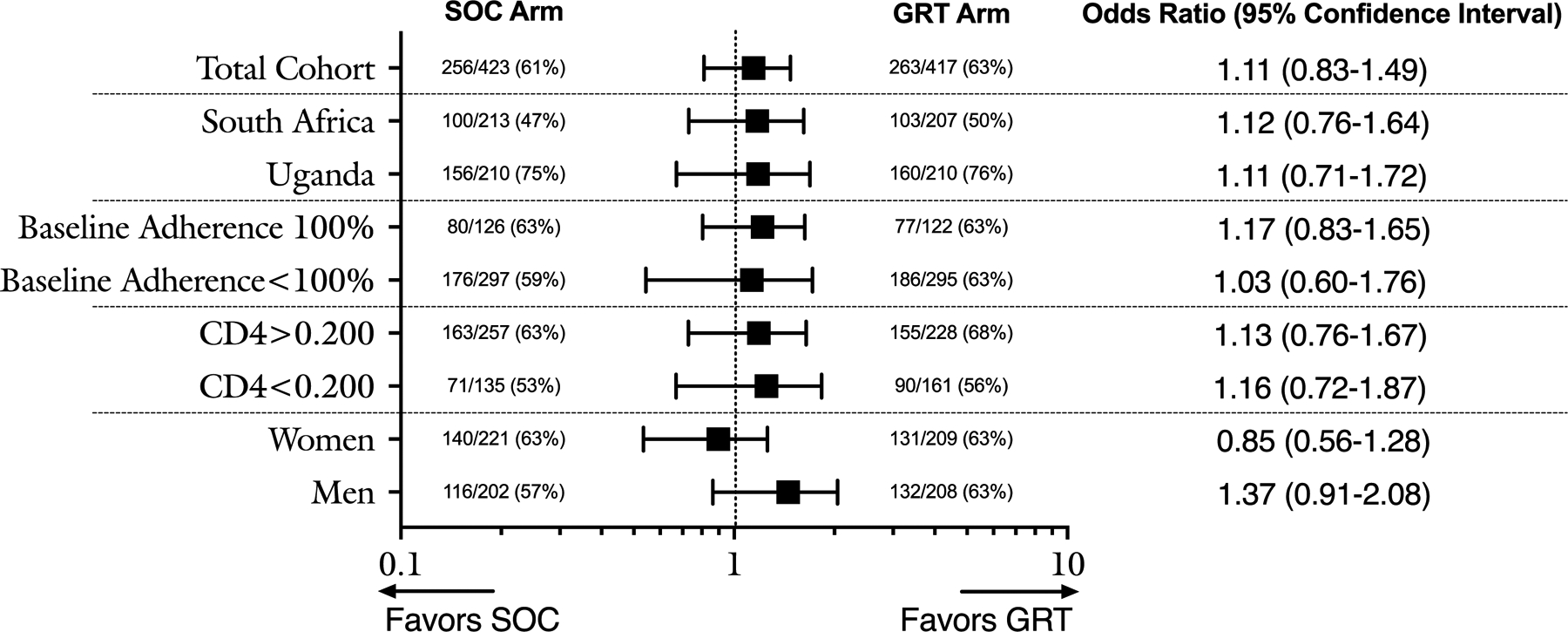
Results: The trial enrolled 840 persons, divided equally between countries. Approximately half (51%) were women. Most (72%) were receiving a regimen of tenofovir, emtricitabine, and efavirenz at enrollment. The rate of virologic suppression did not differ 9 months after enrollment between the GRT group (63% [263 of 417]) and SOC group (61% [256 of 423]; odds ratio [OR], 1.11 [95% CI, 0.83 to 1.49]; P = 0.46). Among participants with persistent failure (HIV RNA viral load ≥1000 copies/mL) at 9 months, the prevalence of drug resistance was higher in the SOC group (76% [78 of 103] vs. 59% [48 of 82]; OR, 2.30 [CI, 1.22 to 4.35]; P = 0.014). Other secondary outcomes, including 9-month survival and retention in care, were similar between groups.
Limitation: Participants were receiving nonnucleoside reverse transcriptase inhibitor-based therapy at enrollment, limiting the generalizability of the findings.
Conclusion: The addition of GRT to routine care after first-line virologic failure in Uganda and South Africa did not improve rates of resuppression.
Primary funding source: The President's Emergency Plan for AIDS Relief and the National Institute of Allergy and Infectious Diseases.
Conflict of interest statement
Figures
Comment in
-
Managing HIV Treatment Failure: Time to REVAMP?Ann Intern Med. 2021 Dec;174(12):1753-1754. doi: 10.7326/M21-3903. Epub 2021 Oct 26. Ann Intern Med. 2021. PMID: 34698505 No abstract available.
References
-
- Palombi L, Marazzi MC, Guidotti G, et al. ; DREAM Program. Incidence and predictors of death, retention, and switch to second-line regimens in antiretroviral-treated patients in sub-Saharan African sites with comprehensive monitoring availability. Clin Infect Dis. 2009;48:115–122. - PubMed
-
- Quinn TC, Wawer MJ, Sewankambo N, et al. ; Rakai Project Study Group. Viral load and heterosexual transmission of human immunodeficiency virus type 1. N Engl J Med. 2000;342:921–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical